Magnesium & the Pineal Gland: Best Forms, Dosage + Protocol
By Marcus Hale·
Magnesium and the Pineal Gland: How It Works, Best Types & Dosage Guide
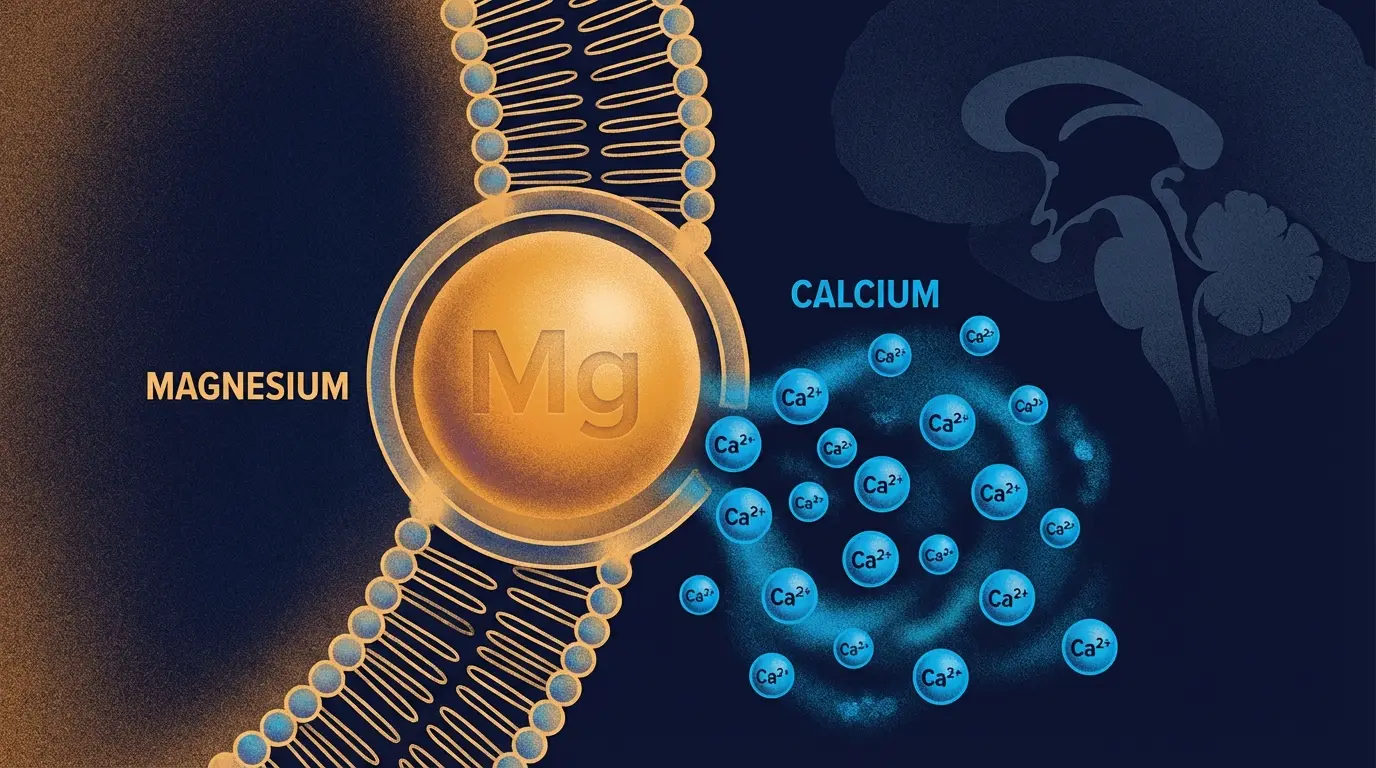
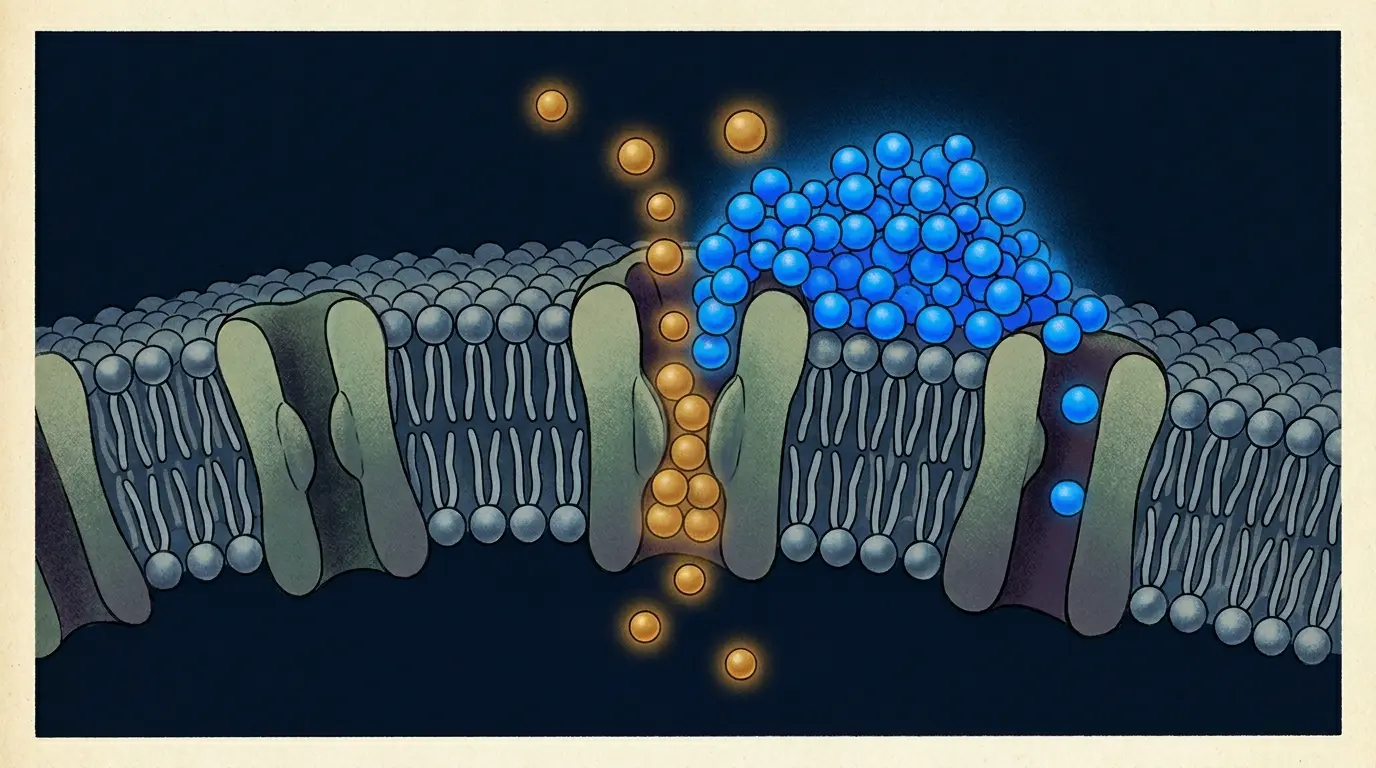
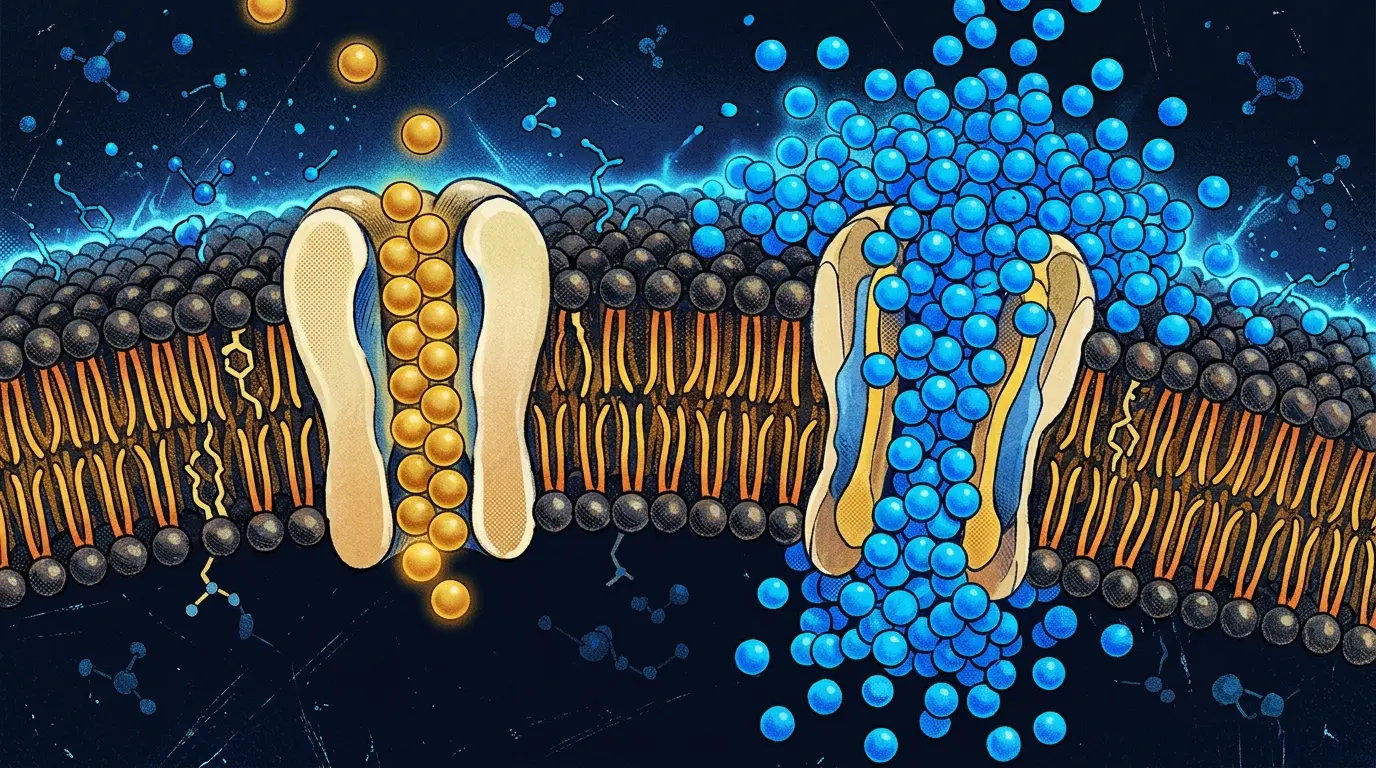
Magnesium and calcium are physiological antagonists — they compete for the same ion channels inside pineal cells. Deficiency in one mineral opens the door for the other.
You’ve probably read that your pineal gland is calcified. Most articles stop there. Or jump straight to a supplement recommendation. What they skip is the one mineral that directly competes with calcium at the cellular level. Magnesium doesn’t get talked about in the context of the pineal gland because it’s not exotic. It’s not a rainforest extract or an ancient Ayurvedic compound. It’s a mineral roughly 40% of American adults don’t get enough of. This article covers the actual mechanism, the forms that matter, the forms that don’t, and a nightly protocol you can start tonight.
What Does the Pineal Gland Do? (And Why Calcification Matters)
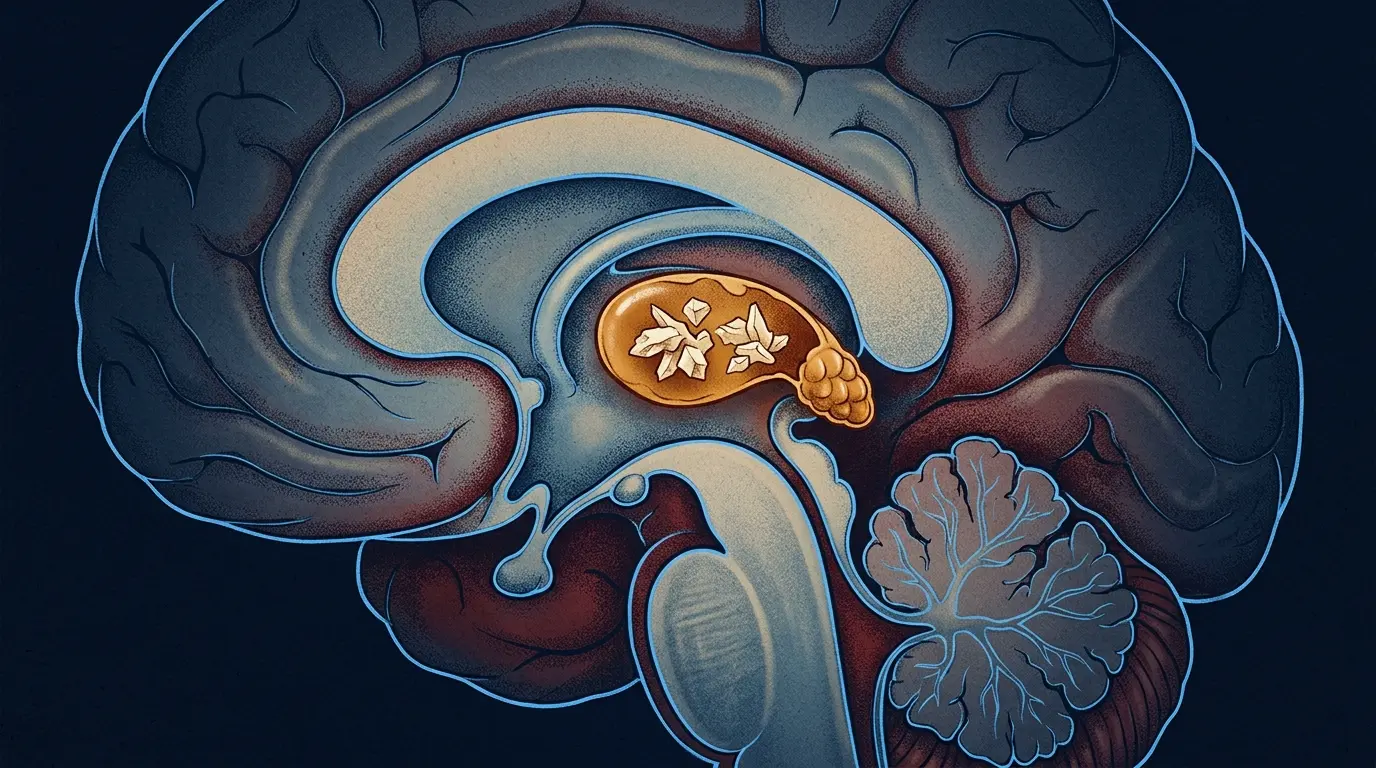
The pineal gland is a pea-sized endocrine structure sitting near the center of your brain. Its primary job: converting serotonin into melatonin when darkness hits, signaling your body to wind down and sleep. Descartes called it “the seat of the soul” in 1649 — which tells you how long humans have suspected this tissue mattered, even when they had no idea what it actually did.
The complication is that the pineal gland has the highest rate of calcification of any tissue in the brain. We’re talking calcium-phosphate and calcite crystals forming in the gland over time, visible on standard X-rays in roughly a third of children by age 11, and in over 70% of adults above 40 in Western populations. As calcification progresses, the gland’s ability to respond to light-dark signals degrades. Less melatonin. Poorer sleep. A gland that’s supposed to be running the show, running quiet instead.
If you’ve been researching pineal decalcification, this is the mineral-level explanation you probably haven’t found yet.
Pineal calcification is visible on standard X-rays — present in roughly a third of children by age 11 and in over 70% of adults above 40 in Western populations (PMC, 2014).
How Does Magnesium Affect the Pineal Gland?
Here’s what’s actually happening at the cellular level, and why this is different from the generic “magnesium is good for your brain” talking point you’ve seen everywhere.
Magnesium and calcium are physiological antagonists. They compete for the same ion channels. When intracellular magnesium is adequate, it physically blocks calcium from accumulating inside cells, pineal cells included. When magnesium is deficient, calcium moves in unchecked. That elevated intracellular calcium environment is exactly what creates the conditions for mineral crystallization. Romani (2011), in a review of cellular magnesium homeostasis published in Archives of Biochemistry and Biophysics, documented this carefully: magnesium regulates Ca²⁺ concentrations in cells, and deficiency produces a hypercalcemic intracellular state that promotes tissue mineralization.
That mechanism alone is worth your attention.
Magnesium regulates Ca²⁺ concentrations in cells — deficiency produces a hypercalcemic intracellular state that promotes tissue mineralization (Romani, Archives of Biochemistry and Biophysics, 2011).
But there’s a second pathway specific to the pineal gland. The enzyme N-acetyltransferase (NAT) is the rate-limiting step in melatonin synthesis — it converts serotonin toward melatonin. Research going back to Klein and colleagues in the early 1970s established that NAT activity is sensitive to electrolyte signaling, magnesium included. Deficient magnesium doesn’t just create conditions for calcification. It may reduce the enzymatic efficiency of the very process that produces your sleep hormone.
Magnesium deficiency creates a hypercalcemic intracellular environment in pineal cells — the same condition that drives calcium-phosphate crystallization — while simultaneously reducing activity of N-acetyltransferase, the rate-limiting enzyme in melatonin synthesis.
To be precise: the chain from magnesium deficiency to reduced NAT activity to lower melatonin has been established in animal models and biochemical reviews. Human data shows that magnesium supplementation raises melatonin levels — Abbasi et al. (2012) demonstrated this in a double-blind trial — though the exact mechanism in living humans hasn’t been isolated. The effect is real. The precise pathway still has inferential steps.
Is Magnesium Good for the Pineal Gland?
Yes — magnesium is one of the most directly relevant minerals for pineal gland health, and the mechanism is specific, not vague.
By competing with calcium at the ionic level, magnesium may help reduce the intracellular calcium accumulation that sets the stage for pineal calcification. By supporting NAT enzyme activity, it supports the enzymatic pathway that produces melatonin. These aren’t separate benefits. They’re two aspects of the same underlying biochemistry. A pineal gland with adequate magnesium has less calcium pressure inside its cells and a more functional melatonin-production line.
What magnesium won’t do: reverse existing calcification overnight. That’s a slower process, and no supplement erases crystals that are already there. The more accurate framing is that magnesium may help prevent further calcium accumulation and support the functional tissue that remains. That’s a smaller claim. It’s also an honest one.
What Type of Magnesium Is Best for the Pineal Gland?
Not all magnesium supplements reach the brain, and that distinction matters enormously when you’re targeting the pineal gland specifically.
Form
BBB Penetration
Bioavailability
Best For
Price
L-Threonate
✅ High
High
Pineal-specific + cognition
$$$
Glycinate
❌ Limited
High
Sleep + gut-friendly
$$
Citrate
❌ Low
Medium
Budget option
$
Only Magnesium L-Threonate (Magtein®) demonstrated elevated cerebrospinal fluid magnesium in controlled models — citrate, chloride, and gluconate failed to cross the CNS (Slutsky et al., Cell, 2010).
Magnesium L-Threonate — The Brain-Penetrating Form
Magtein® (the patented form of magnesium L-threonate) is the only form of magnesium demonstrated to raise magnesium concentrations in cerebrospinal fluid. The landmark study comes from Slutsky et al. (2010), published in Cell: when researchers tested multiple magnesium forms in animal models, only L-threonate elevated brain magnesium levels. Citrate, chloride, gluconate: none of them crossed into the central nervous system effectively.
For pineal-specific support, this matters. If the goal is getting magnesium to the tissue that needs it, L-Threonate is the only form with direct evidence of CNS penetration.
The biohacking community has basically made L-Threonate the default answer for anything brain-related. I understand why. But if you’re primarily after better sleep and you’re not flush with cash, read the next section before you order the expensive option.
Magnesium Glycinate — Best for Sleep and Absorption
Glycinate is chelated magnesium, bound to the amino acid glycine, which gives it high bioavailability and a gentle profile for the digestive tract. It doesn’t have the brain-penetration data that L-Threonate has. What it does have: solid evidence for improving sleep quality, and glycine carries sedative properties that work alongside melatonin rather than independently of it.
For most people running a nightly protocol, this is the practical call. Effective, well-tolerated, reasonably priced.
Magnesium Citrate — Budget Option
Citrate is fine for correcting a general magnesium deficiency. Meaningful brain penetration: no. If your magnesium status is genuinely low and budget is tight, start here and upgrade later. For pineal-targeted support, it’s the wrong tool.
Does Magnesium Threonate Cross the Blood-Brain Barrier?
Yes — magnesium L-threonate (Magtein®) is the only form shown to raise magnesium levels in cerebrospinal fluid in controlled studies.
I’ll be honest: I spent a while framing this section around the BBB argument before catching an important error. The pineal gland doesn’t actually sit behind the blood-brain barrier. It’s one of the circumventricular organs — it samples blood directly. Which means the BBB-crossing argument is more relevant for structures like the hippocampus and cortex, the targets in Slutsky et al.’s original cognition research. For the pineal specifically, what matters is serum magnesium availability and intracellular competition with calcium.
That said, the L-Threonate advantage holds. Human trials using Magtein® have confirmed cognitive improvements consistent with elevated CNS magnesium, even though no human study has directly measured cerebrospinal magnesium via lumbar puncture. And higher circulating magnesium means more available to compete with calcium in pineal cells.
Magnesium and Melatonin: The Sleep-Pineal Connection
The link between magnesium and melatonin isn’t indirect. Magnesium supports the enzymatic steps that convert serotonin to melatonin, particularly NAT activity. Without adequate magnesium, that conversion runs less efficiently.
Abbasi et al. (2012) ran an 8-week double-blind, placebo-controlled trial with 46 elderly insomnia patients. The magnesium group fell asleep faster, slept longer, and showed significantly elevated serum melatonin levels versus placebo. Nielsen et al. (2010) found similar improvements in sleep quality and inflammatory markers in adults with low magnesium status. These aren’t mechanistic studies. They don’t isolate the NAT pathway in humans, but the pattern holds up regardless of which study you’re reading.
The practical implication: if your magnesium is low, your melatonin may be low for reasons that have nothing to do with light exposure or screen time. Check the deficiency before you blame the habit.
Want to combine this with a nighttime decalcification protocol? The timing of supplementation matters, and there’s more detail on that below.
How Much Magnesium Should You Take for Pineal Gland Health?
The safe supplemental range is 200–400 mg per day for most adults. The Institute of Medicine sets the Tolerable Upper Intake Level for supplemental magnesium at 350 mg/day — above that, gastrointestinal effects (loose stools, cramping) become likely. If you have kidney disease or impaired renal function, talk to a healthcare provider before supplementing at any dose.
Dose: 200–300 mg elemental magnesium (not the total weight of the compound — read the label)
Timing: 30–60 minutes before bed, in a darkened room
Duration: Sleep improvements are typically noticeable within 1–2 weeks; any impact on long-term calcium dynamics is a months-long process, not a week-long one
One caveat: there’s no clinical study defining a “pineal-specific dose” of magnesium. The 200–400 mg range is based on sleep and deficiency research, not on a study that measured pineal calcification as an endpoint. That study doesn’t exist yet. The dosage is safe and evidence-based — but anyone claiming a precise “pineal dose” is getting ahead of the data.
Abbasi et al. (2012): 8-week double-blind trial, 46 patients — magnesium group showed significantly elevated serum melatonin, faster sleep onset, and longer sleep duration versus placebo.
Want a Complete Pineal Formula?
If you’d rather not manage individual supplements, some formulas combine magnesium with other compounds studied for pineal and sleep support.
Pineal Guardian includes magnesium alongside other pineal-supportive ingredients in a single daily formula — useful if you want convenience over the build-your-own-stack approach. See the full Pineal Guardian formula breakdown before deciding.
Timing matters: taking magnesium 30–60 minutes before bed aligns supplementation with the body’s natural melatonin production window — the window NAT enzyme activity peaks.
Frequently Asked Questions
Is magnesium good for the pineal gland?
Yes. Magnesium competes with calcium in ionic channels, reducing intracellular calcium buildup — the primary driver of pineal calcification. It also activates the NAT enzyme that produces melatonin, making it pineal-specific in its benefits.
What type of magnesium is best for the pineal gland?
Magnesium L-Threonate is the best choice for pineal-specific support because it is the only form clinically shown to raise magnesium levels in cerebrospinal fluid. Magnesium Glycinate is a strong second option for sleep support and general absorption.
Does magnesium threonate cross the blood-brain barrier?
Yes. Magnesium L-Threonate (Magtein®) is the only magnesium form demonstrated to elevate cerebrospinal fluid magnesium concentrations in studies, while other forms like citrate, glycinate, and chloride could not achieve the same effect.
How much magnesium should I take for pineal gland health?
A safe and effective dose is 200–400 mg per day of Magnesium Glycinate or L-Threonate. Take it 30–60 minutes before bed to align with your body's natural melatonin production window. Always consult a healthcare provider if you have kidney issues.
Marcus Hale is an independent researcher and former clinical neuroscientist. The content on PinealCode.com is for informational purposes only and does not constitute medical advice.
Medical Disclaimer: The content on
PinealCode.com is for informational and educational purposes only. Nothing here
constitutes medical advice, diagnosis, or treatment. Always consult a qualified
healthcare provider before making changes to your health regimen.
Marcus Hale
Independent Researcher · Former Clinical Neuroscientist
I spent 12 years in clinical neurology before the questions got more interesting
than the answers. PinealCode is where I document what I find at the intersection
of brain science and consciousness.