Bentonite Clay and the Pineal Gland: Does It Decalcify?
By Marcus Hale··Updated March 26, 2026
The wellness internet has decided that bentonite clay decalcifies your pineal gland. Thousands of people are mixing gray powder into water every morning because of it.
The actual chemistry tells a different story. Not a worse story. More precise.
Bentonite clay is a real thing with real mechanisms. It binds heavy metals in the digestive tract. That’s documented, peer-reviewed, not controversial. The question is whether “binds heavy metals in the gut” equals “decalcifies a gland in the center of your brain.” Those are not the same claim. They’re not even in the same category.
Here’s what the evidence actually shows. And where it runs out completely.
Can Bentonite Clay Decalcify the Pineal Gland?
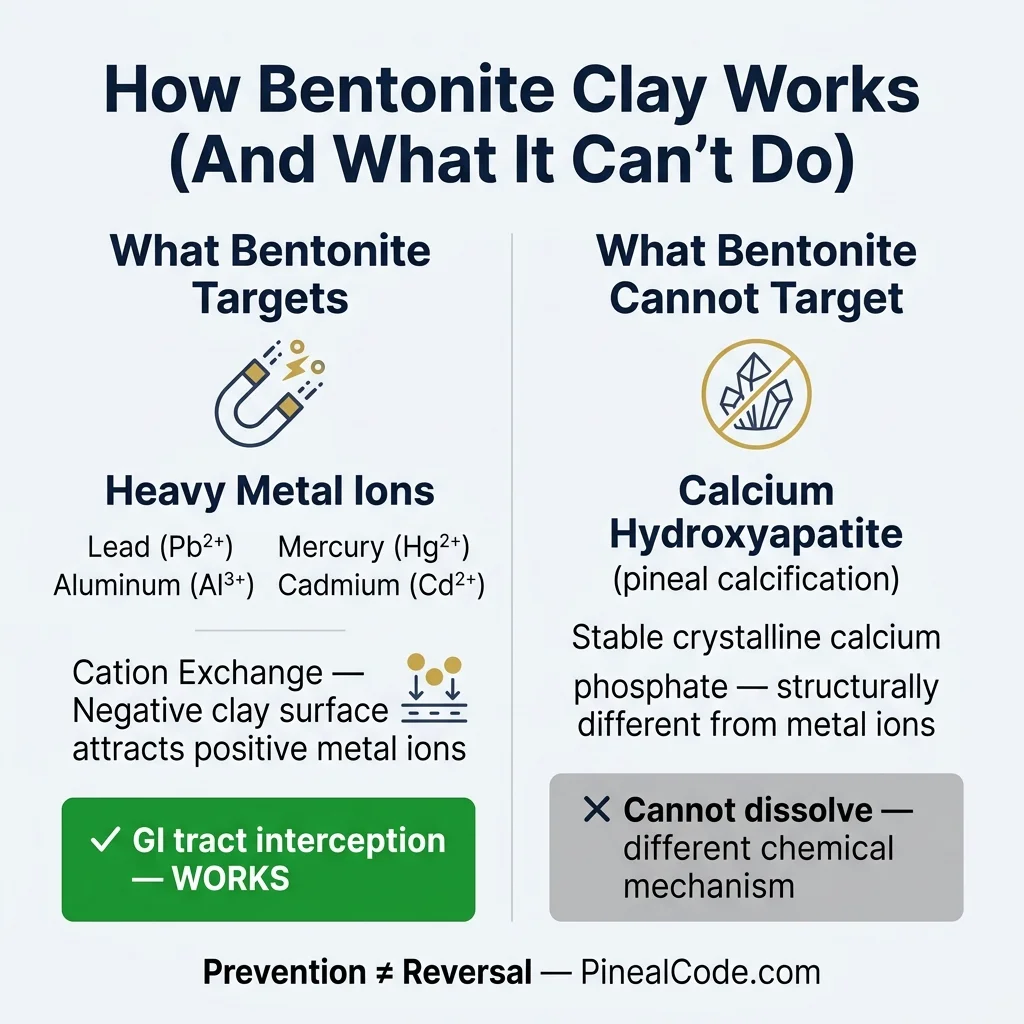
No — not directly, and the chemistry explains why. Bentonite is an aluminosilicate clay that works through cation exchange: it carries a negative surface charge and attracts positively charged metal ions like lead, mercury, aluminum, and cadmium. Pineal gland calcification is primarily calcium hydroxyapatite: a stable crystalline calcium phosphate compound. That’s a different chemical target entirely. Bentonite’s adsorption mechanism doesn’t dissolve hydroxyapatite deposits. Structurally, it can’t.
But here’s where it gets more interesting than a flat “no.”
Heavy metals, particularly lead and aluminum, are found in elevated concentrations in calcified pineal tissue. The 2002 work from Baconnier et al. identified distinct crystal formations in human pineal epithelium, and the broader literature on pineal calcification implicates metal accumulation as a contributing factor alongside fluoride and aging. If bentonite clay reduces the systemic load of those metals before they reach neural tissue, intercepting them in the GI tract before absorption, that’s not decalcification. That’s upstream prevention.
Prevention and reversal are different things. Be precise about which one you’re pursuing.
Bentonite clay works by cation exchange — its negatively charged surface attracts positively charged heavy metal ions like lead and aluminum in the gut. It does not dissolve calcium hydroxyapatite deposits already formed in pineal tissue.
Does Bentonite Clay Remove Fluoride from the Body?
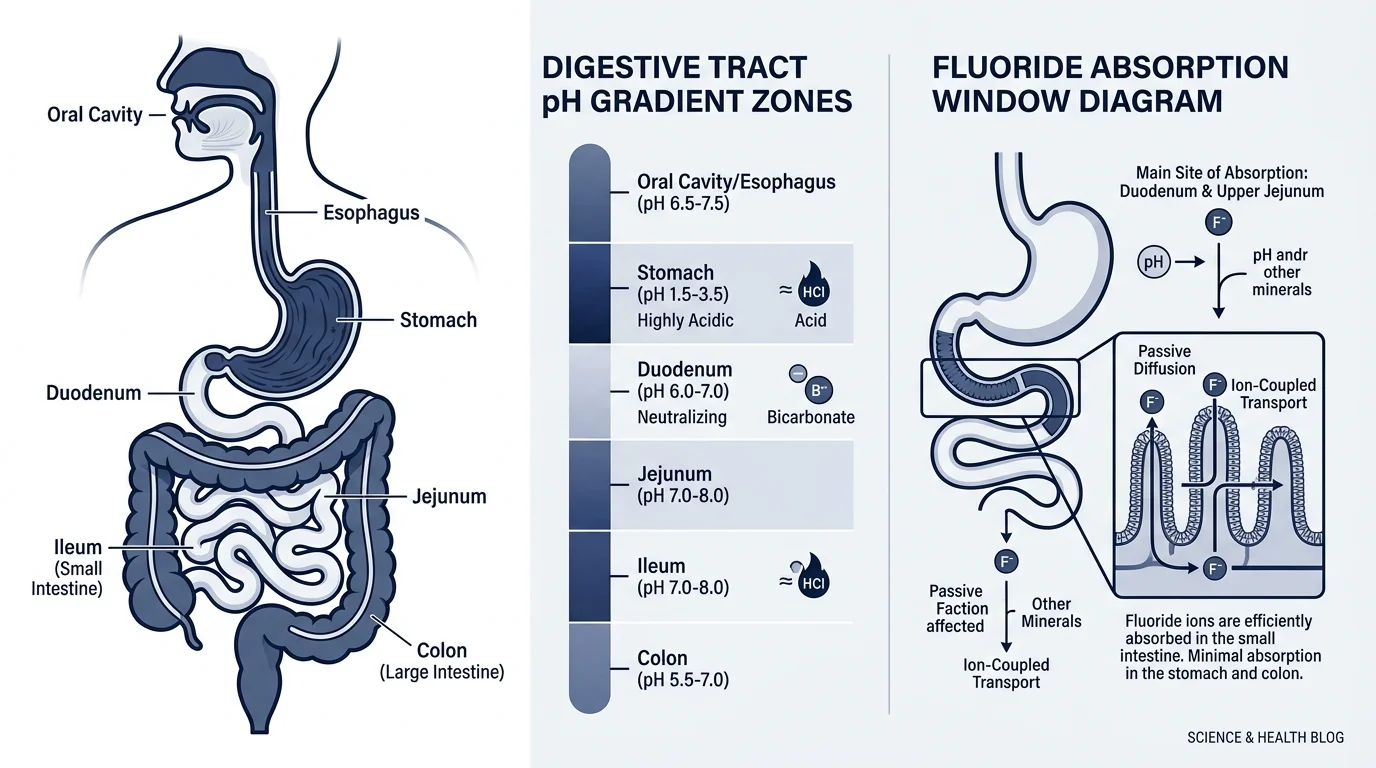
Partially, and only under specific conditions. In water purification studies, modified bentonite achieves fluoride adsorption, but optimal efficiency occurs at pH 3, which corresponds to stomach-level acidity. By the time bentonite reaches the small intestine (pH 6–7.5), fluoride binding capacity drops significantly.
More important: fluoride already incorporated into hydroxyapatite in pineal tissue is chemically bound into a crystal lattice. Bentonite in your digestive tract cannot reach it. That fluoride is gone. Structurally integrated. The window where bentonite could theoretically intercept fluoride is during absorption, before it enters circulation. Whether that actually reduces pineal fluoride burden in humans has never been measured.
Bentonite clay reduces fluoride absorption from water at stomach pH, but cannot remove fluoride already crystallized into calcium hydroxyapatite deposits in the pineal gland — a distinction no human clinical trial has yet quantified.
That gap in the literature isn’t a conspiracy. It’s just that nobody has funded this study. It probably won’t make anyone money.
Bentonite clay’s fluoride binding capacity peaks at stomach-level acidity (pH 3) and drops significantly in the small intestine (pH 6–7.5). Fluoride already crystallized into pineal tissue is completely unreachable by gut-based enterosorbents.
How Bentonite Clay Actually Affects Brain Health
Descartes called the pineal gland the seat of the soul. Three hundred years later we’re still not fully sure what it does beyond melatonin production. We are fairly sure we’d prefer it uncalcified.
Lead, mercury, and aluminum accumulate preferentially in neural tissue. The brain is 60% fat, and certain heavy metals have a strong affinity for lipid-rich environments. The pineal gland, small, heavily vascularized, and sitting outside the blood-brain barrier in several physiological models, is particularly exposed.
Here’s what bentonite can plausibly do: a 2025 study in Scientific Reports showed activated calcium bentonite adsorbs up to 13 mg/g of lead and 14 mg/g of copper from aqueous solution. These are water treatment numbers, not human gut numbers. But the mechanism is real. If even a fraction of that binding capacity operates in the GI tract, you’re reducing the amount of lead and aluminum entering circulation in the first place.
Less circulating lead. Less available for neural deposition. Less potential contribution to calcification over decades.
That’s the honest version of the claim.
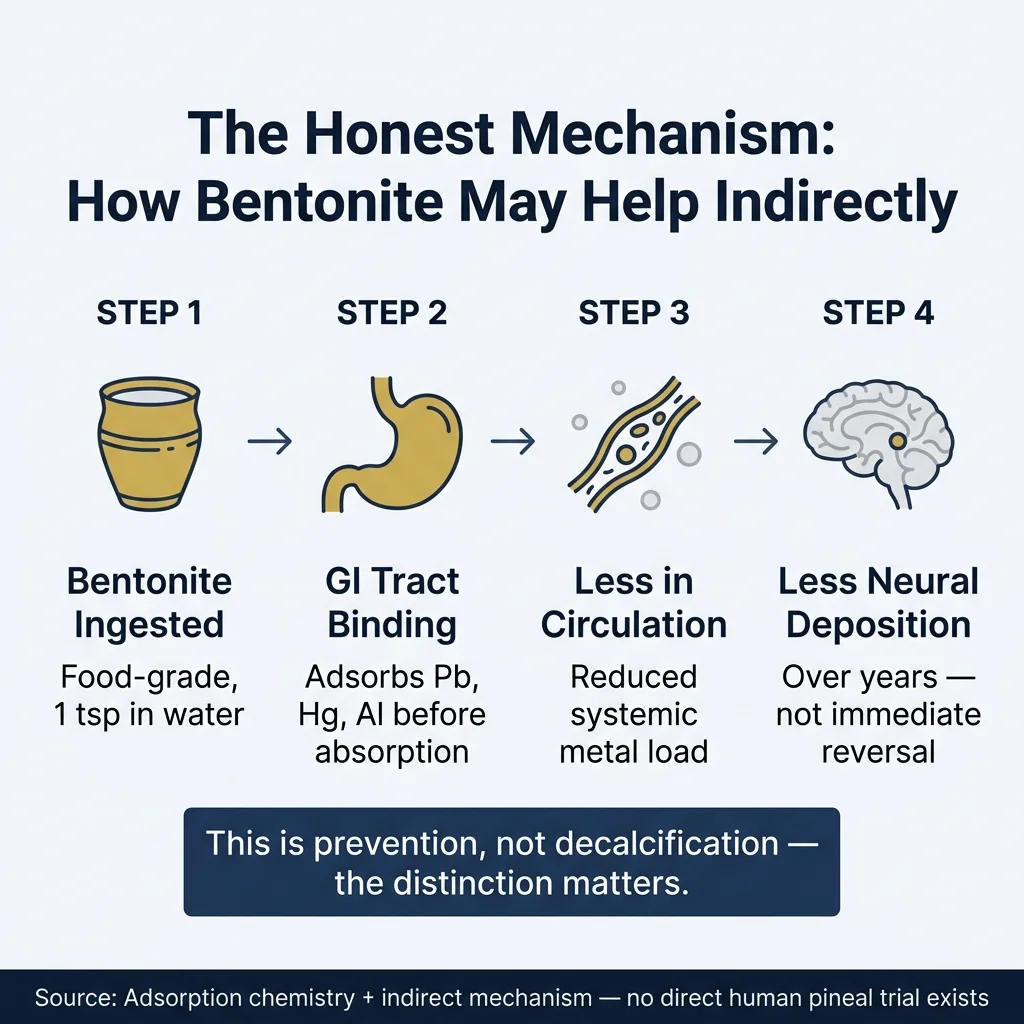
The honest mechanism: bentonite clay intercepts heavy metals in the GI tract → less lead and aluminum entering circulation → less available for neural deposition over decades. Prevention, not reversal.
There’s a paradox worth sitting with, though. Bentonite’s chemical formula is Al₂O₃·4SiO₂·H₂O. It naturally contains aluminum as a structural component. Whether food-grade bentonite releases bioavailable aluminum during GI transit, and whether that offsets any heavy metal binding benefit, has not been adequately studied in humans. Nobody can give you a clean answer on this yet.
Is Bentonite Clay Good for the Brain?
Here’s what I can say with reasonable confidence: the benefit mechanism is real. Reduced GI absorption of heavy metals is biologically sound and backed by adsorption chemistry, even without direct human data.
The risk side is trickier. Aluminum leaching from the clay itself is plausible and equally unquantified. I genuinely don’t know which effect dominates in practice. Neither does anyone else, because the study hasn’t been done.
What we do know is that food-grade calcium bentonite has established safety for short-term oral use as an enterosorbent, with the most rigorous safety data coming from aflatoxin-binding research out of Texas A&M. That’s not the same as a long-term heavy metal protocol. Different dose, different duration, different intended mechanism.
If you’re going to use it, the grade distinction matters more than the brand.
How to Use Bentonite Clay for Pineal Detox
Oral Protocol
One teaspoon of food-grade calcium bentonite stirred into 8–12 oz of water. Drink it, don’t chew it, which sounds obvious until you’ve seen what people do online. Use a non-metal spoon; the clay interacts with metal utensils. Let it sit a few minutes to hydrate before drinking.
Timing
Take it at least 1–2 hours away from food, supplements, and medications. This is not optional. Bentonite adsorbs indiscriminately: it doesn’t distinguish between lead and your thyroid medication. It will bind both. If you take prescription drugs, talk to a doctor before using any enterosorbent clay.
Duration
Two to four weeks, then stop for a while. Continuous daily use has no clinical safety data behind it. The wellness community runs longer, sometimes indefinitely. I’d want more human data before committing to that. Constipation is also the most common complaint in community forums about extended use. That alone should give you pause.
Correct oral protocol: 1 tsp food-grade calcium bentonite in 8–12 oz water, non-metal spoon, 1–2 hours from all medications and supplements. Use for 2–4 weeks with breaks. Industrial grades are not safe for internal use.
What to Combine With
Bentonite targets heavy metals. For fluoride specifically, tamarind extract has stronger evidence. For calcium deposits, K2+D3 addresses the underlying deposition mechanism more directly. If you want to cover all the bases on pineal health, bentonite is one tool, not the whole protocol. (See the full comparison below.)
Food-Grade vs. Industrial Grade
This distinction matters more than most people realize. Industrial bentonite goes into drilling fluids, cat litter, and construction. Contaminant loads differ. Look for “food-grade” or “USP-grade” on the label, with third-party testing for heavy metals. Yes, the clay that removes heavy metals needs to be tested for heavy metals. That’s the world we live in.
Bentonite fills a specific niche, heavy metal interception, that the other methods don’t address. It’s not competing with K2+D3. They’re solving different parts of the same problem.
What This Means for You
Bentonite clay does not decalcify your pineal gland. That claim outpaces the evidence by about three logical steps.
What it does, if food-grade, used short-term, and timed correctly away from medications, is reduce heavy metal absorption in the GI tract. Over time, less lead and aluminum entering circulation means less available for neural deposition. That’s a real mechanism. It’s just slower, more indirect, and less dramatic than “open your third eye.”
It’s a prevention tool, not a reversal. Part of a protocol, not a solution.
If you want to start somewhere concrete: fix your sleep first. Melatonin production, the primary measurable output of the pineal gland, is almost entirely dependent on sleep hygiene. No clay protocol outperforms eight hours of dark, consistent sleep. That’s not a romantic answer. It’s just what the data says.
The informed approach: food-grade only, third-party tested for heavy metals, timed away from medications, 2–4 weeks maximum. Use it as one layer of a protocol — not as a standalone solution.
Frequently Asked Questions
Can bentonite clay decalcify the pineal gland?
Not directly. Bentonite clay adsorbs heavy metals but does not dissolve calcium hydroxyapatite deposits. It may support pineal health by reducing heavy metal accumulation that contributes to calcification over time.
Does bentonite clay remove fluoride from the body?
Partially. Bentonite can adsorb fluoride in the digestive tract before absorption, most effectively at stomach-level acidity. It cannot remove fluoride already incorporated into calcified pineal tissue.
Is bentonite clay safe to eat?
Food-grade bentonite in small doses (1 tsp/day) appears safe for short-term use based on enterosorbent research. Avoid industrial grades. Do not take alongside medications — it adsorbs pharmaceuticals as readily as heavy metals.
What clay is best for pineal gland detox?
Food-grade calcium bentonite and zeolite are most studied for internal heavy metal binding. Neither decalcifies the pineal directly — they support by intercepting metals before systemic absorption.
How long should I use bentonite clay for detox?
Most protocols run 2–4 weeks with breaks. Continuous use is not supported by clinical safety data. Take 1–2 hours away from food, supplements, and medications.
Marcus Hale is an independent researcher and former clinical neuroscientist. The content on PinealCode.com is for informational purposes only and does not constitute medical advice.
Medical Disclaimer: The content on
PinealCode.com is for informational and educational purposes only. Nothing here
constitutes medical advice, diagnosis, or treatment. Always consult a qualified
healthcare provider before making changes to your health regimen.
Marcus Hale
Independent Researcher · Former Clinical Neuroscientist
I spent 12 years in clinical neurology before the questions got more interesting
than the answers. PinealCode is where I document what I find at the intersection
of brain science and consciousness.