Pineal Gland Calcification: Doctors Say Permanent — But 3 Studies Disagree
By Marcus Hale·
Can Pineal Gland Calcification Be Reversed? What the Evidence Says
Yes — but with important caveats. I’m leading with those caveats because most content in this space skips them entirely to sell you something.
Can pineal gland calcification be reversed? Partially, in some people, under certain conditions. How far it’s reversible depends on how advanced the calcification is and how long it’s been building. Light microdeposits? The biological levers we have are real. Decades of dense fluorapatite crystal formation? Full structural reversal is probably not on the table — but stopping progression and supporting the functional tissue that remains absolutely is.
Two other things you need upfront: no human clinical trial has measured pineal calcification reversal as a direct endpoint. The evidence chain is built from adjacent science — fluoride excretion studies, soft-tissue calcification biochemistry, the K2/MGP pathway. It’s the strongest thread available. It isn’t a controlled trial. Also: this article focuses on the whether of reversal. For the step-by-step protocol, see our full reversal protocol.
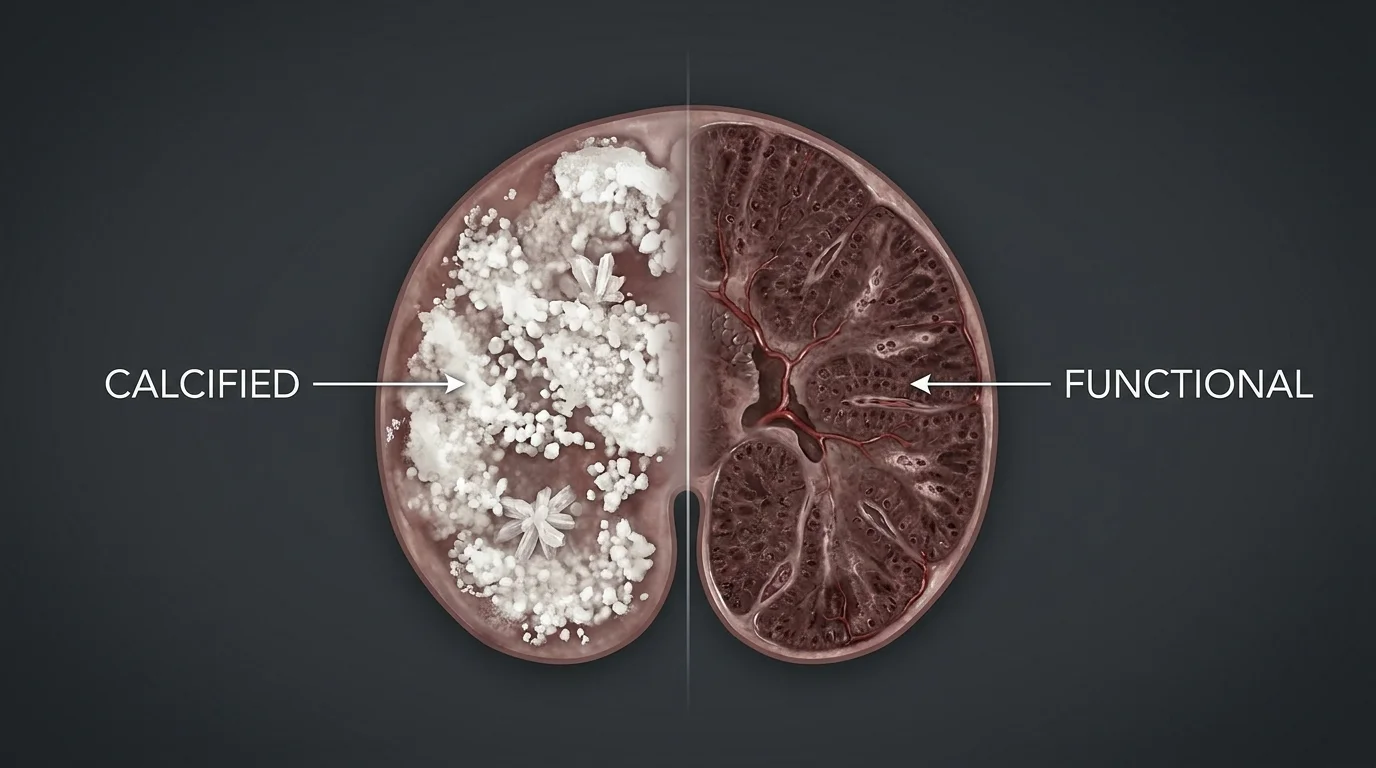
What Type of Calcification Are We Talking About?
Not all pineal calcification is the same thing. Most sites treat it that way. They’re wrong — and the distinction matters before you spend money on a protocol.
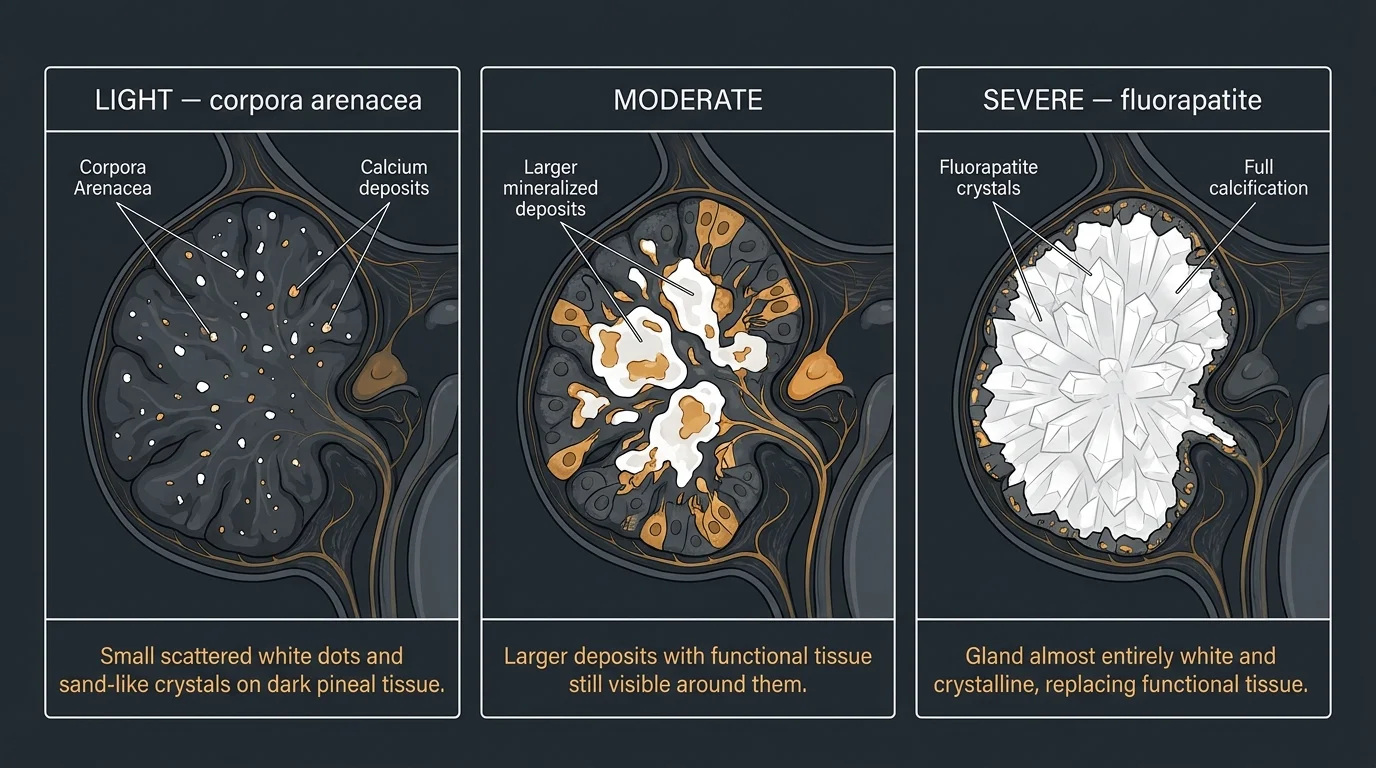
Light calcification — corpora arenacea. Small, laminar deposits of hydroxyapatite and calcium carbonate that build progressively with age. Detectable on standard X-ray or CT, common in adults over 30, and — this is the part that matters — more biologically responsive to intervention. The mineral structure is closer to bone than to crystallized fluoride compound. The chemistry of dissolution is more favorable.
Moderate calcification. Established deposits with functional pineal tissue still present around them. A meaningful portion of your melatonin-producing cells remain intact. This is where a well-executed protocol has the most realistic shot.
Severe/dense calcification. This is the fluorapatite range — the compound formed when fluoride integrates into the mineral matrix. A 2013 materials science study from Plymouth Repository confirmed what basic chemistry predicts: fluorapatite dissolves significantly more slowly than pure hydroxyapatite, and the higher the fluoride substitution, the more resistant to dissolution. Decades of fluoride exposure compounding into crystalline deposits puts you here. The realistic goal is halting progression, not full dissolution.
A 2023 systematic review found pooled global prevalence of pineal calcification at 61.65% in adults. The heterogeneity between studies was extreme — I² of 97.7% — which tells you this isn’t a uniform condition across populations.
Three types of pineal calcification with different reversal potential. Light deposits are the most biologically responsive; severe fluorapatite formation is the hardest to reverse.
How Do You Know How Calcified Yours Is?
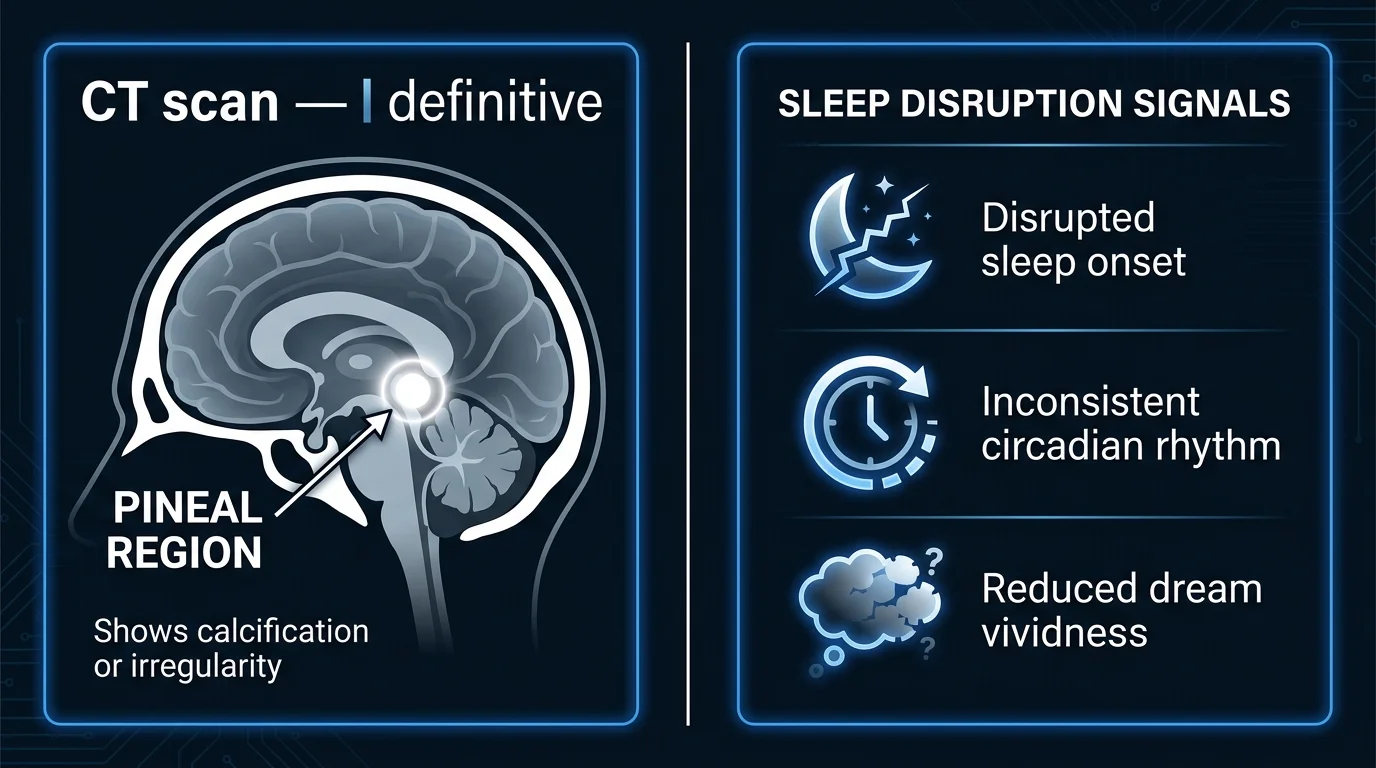
CT scan is the only definitive answer. It visualizes the deposits directly. Most people don’t have a medical indication for one, and I’m not suggesting you manufacture one.
The practical proxy is sleep architecture. Kunz et al. (1999) found that degree of pineal calcification correlated negatively with melatonin amplitude and positively with daytime drowsiness in a pilot study of 22 subjects. A larger automated study in 2026 didn’t replicate that correlation after adjusting for demographics. I’m presenting both — not cherry-picking the one that fits the narrative. What that means practically: disrupted sleep onset, inconsistent circadian rhythms, reduced dream vividness are the signals you actually have access to. They’re imperfect. They’re also what exists without ordering a CT scan.
CT scan is the only direct assessment. Practical proxies — sleep onset, circadian consistency, dream vividness — are the accessible indicators for most people.
What the Research Shows About Reversal
Here’s the honest state of the science.
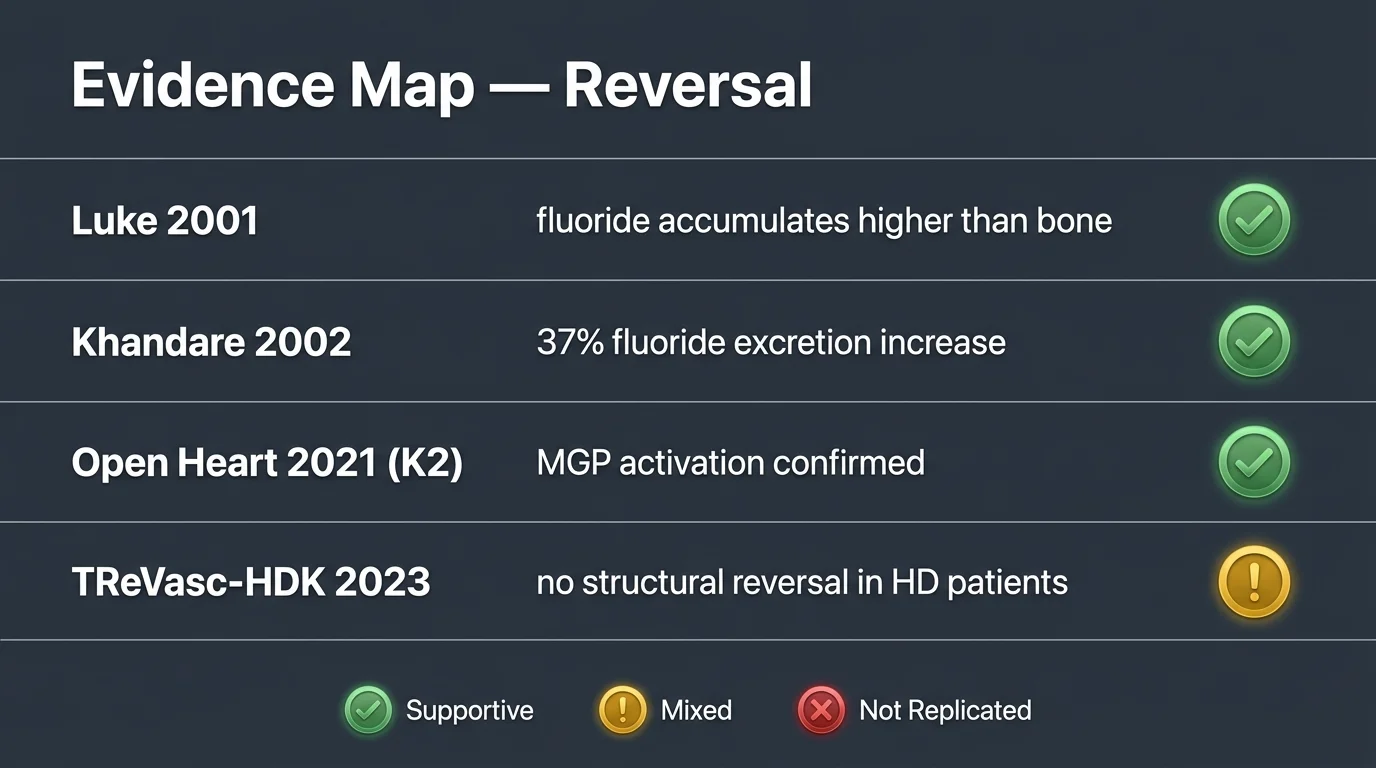
The fluoride problem. Luke (2001, Caries Research) documented fluoride accumulation in the human pineal gland at concentrations of 14–875 mg F/kg — averaging around 300 mg F/kg in older specimens. Comparable to dental enamel. Higher than bone. Higher than any other soft tissue in the body. The mechanism: fluoride integrates into the mineral deposits as fluorapatite — more chemically stable, harder to reverse, than the hydroxyapatite that forms without fluoride exposure.
The tamarind data. Khandare et al. (2002, European Journal of Clinical Nutrition) gave 10g of tamarind daily to 18 children in an endemic fluorosis area in India for 18 days. Urinary fluoride excretion went from 3.5 to 4.8 mg/day — a 37% increase (p<0.001). A 2004 follow-up from the same group found tamarind didn’t just block new absorption: it mobilized fluoride already deposited in bone. That’s the distinction that matters. Chelation of established deposits, not just prevention of new ones.
The honest limits: both studies used children from areas of endemic fluorosis — fluoride body burden far above the typical Western exposure of 0.7 ppm fluoridated tap water. Whether tamarind has the same excretion effect in lower-fluoride populations hasn’t been studied. That gap is real.
The K2/MGP pathway.Matrix Gla Protein (MGP) is the body’s primary biological inhibitor of soft-tissue calcification. When it’s inactive — uncarboxylated, which happens when vitamin K2 is deficient — MGP allows ectopic calcification to proceed unchecked. Seventeen vitamin K-dependent proteins have been identified; MGP is the most potent for soft-tissue regulation.
A 2021 Open Heart (BMJ) review linked K2 MK-7 supplementation to improved MGP activation and cardiovascular calcification outcomes. But the TReVasc-HDK trial (2023, Kidney International Reports) — the most rigorous RCT of K2 in soft-tissue calcification available — administered 360 µg of K2 three times weekly to hemodialysis patients and found no reduction in vascular calcification progression, even as dp-ucMGP improved. Biomarker improvement did not translate to structural reversal.
That result belongs in this article. Omitting it would be the kind of editorial choice that makes this whole space less credible. The K2 mechanism is real. The clinical translation to established, dense calcification in a high-risk population failed in that trial. The calcification stage matters. The population matters.
The honest evidence map for reversal. Tamarind shows fluoride mobilization in human data; K2 activates the right pathway but hasn’t translated to structural reversal in dense-calcification trials.
What Doesn’t Work
Let’s move through this quickly.
Amethyst crystals and orgonite. There’s no biological mechanism by which any external crystal object affects tissue chemistry inside the skull. Zero plausibility.
Lemon water “dissolving” calcium. Citric acid doesn’t cross the blood-brain barrier at concentrations that matter. The pH of a glass of lemon water has no interaction with fluorapatite crystals in your pineal gland. I know that’s not what some people want to hear.
Oil of oregano, turpentine, MMS. No peer-reviewed mechanism for pineal decalcification. Some carry active toxicity risks. We’re not dismissing the intent behind these recommendations. We’re reporting what the evidence doesn’t support — and in the case of MMS, what the evidence actively warns against.
Generic detox supplements. Liver support and broad antioxidant stacks address legitimate physiological goals. They don’t address pineal calcification. The fluoride-MGP-mineral pathway needs targeted interventions, not general wellness protocols.
Four common approaches with no evidence for pineal decalcification. The fluoride-MGP pathway requires targeted interventions — not general wellness products.
How Long Does Reversal Take?
There’s no controlled timeline for pineal decalcification — because no one has run that trial. What we have are adjacent data points that give a realistic frame.
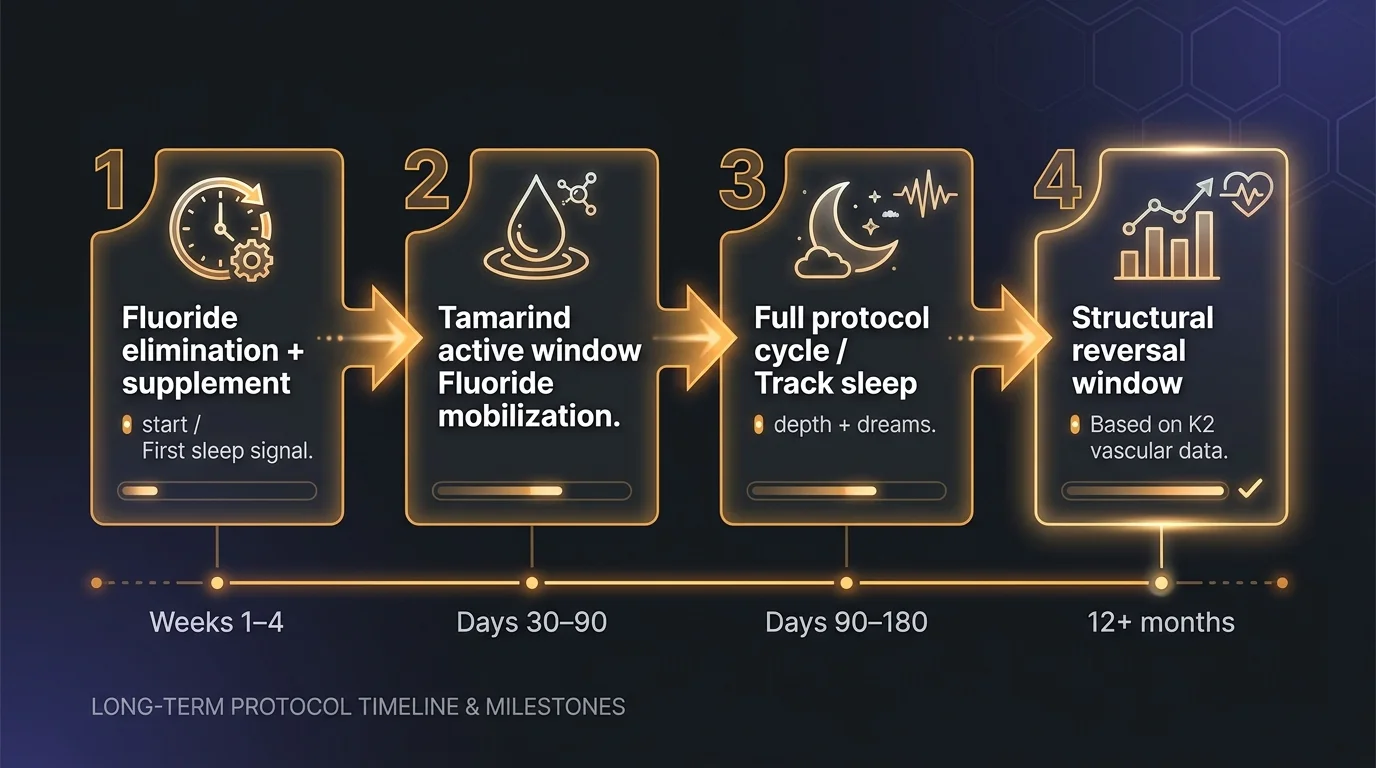
Weeks 1–4. Eliminate fluoride from water and toothpaste. Begin tamarind and K2/D3 supplementation. The first measurable signal most people notice is sleep quality — not because calcification has reversed, but because reducing ongoing fluoride input and activating the MGP pathway lets residual functional tissue operate with less interference. Expectations matter here. This is not “it’s working.” This is “conditions are improving.”
Days 30–90. If Khandare’s tamarind data translates to lower-fluoride populations, urinary fluoride excretion should be elevated during this window — indicating mobilization of stored deposits. This is where the chelation mechanism, if it’s working, is most active. You can’t measure it without a lab. You track sleep depth instead.
90–180 days. A full protocol cycle. Circadian consistency, sleep depth, and dream vividness are the most accessible progress indicators. There’s no blood test that confirms structural change in the pineal specifically. The dp-ucMGP biomarker reflects K2 activity — not pineal calcification status directly.
12+ months. K2 vascular calcification trials use 12–24 month windows to detect structural changes. Modest but real improvements in vascular calcification have been documented over that timeline in non-HD populations — with the TReVasc-HDK caveat already noted. The principle holds across contexts: structural mineral reversal takes years, not weeks.
No pineal-specific trial exists, but adjacent K2 and tamarind data suggest a 90–180 day active window and 12+ months for any structural change. Sleep signals are the accessible progress marker.
The Most Effective Approaches
The data points to these options. Not as a guarantee — as the strongest available starting points.
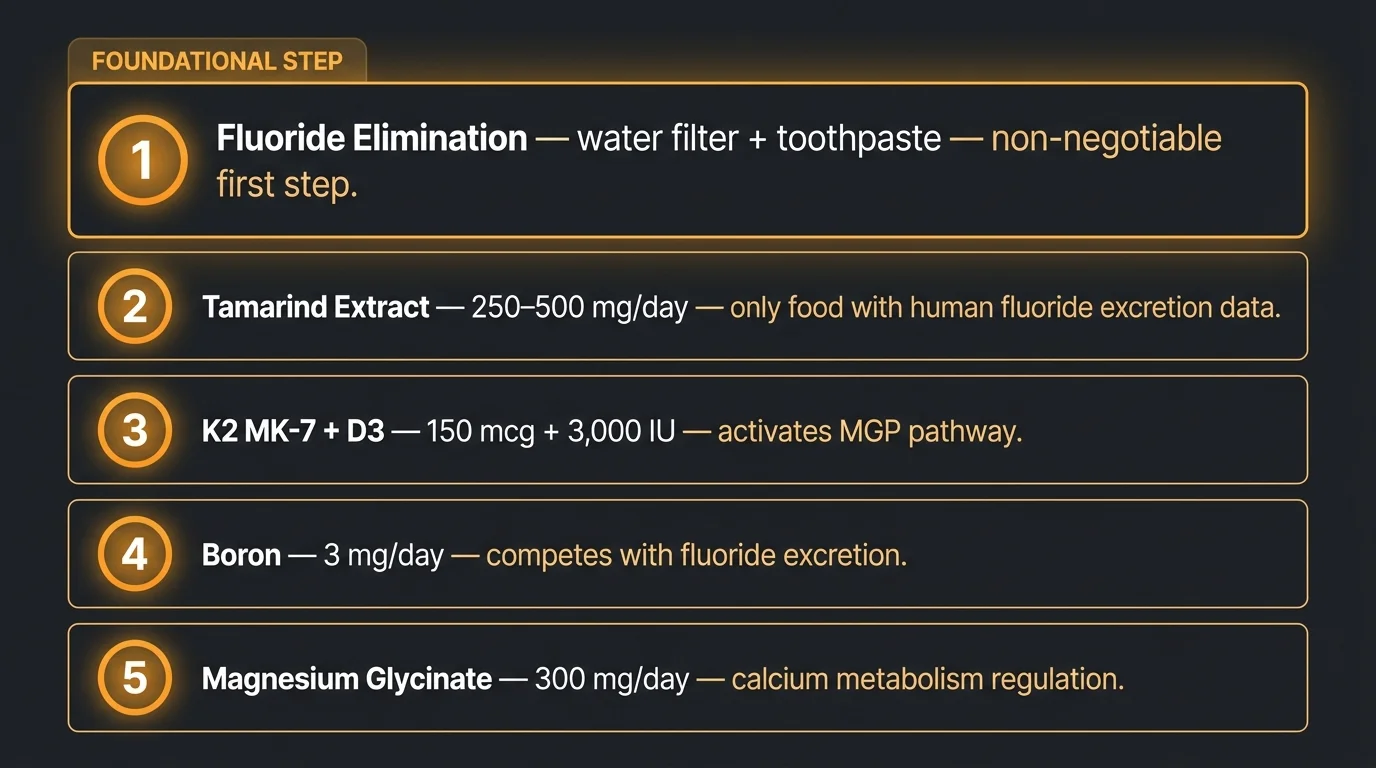
1. Eliminate fluoride first. Before any supplement. This is non-negotiable. You can’t meaningfully address calcification while still loading the gland with the primary mineralizing agent. Reverse osmosis removes fluoride from water; most carbon filters don’t. Switch to fluoride-free toothpaste. These two changes cost almost nothing compared to a supplement stack.
2. Tamarind extract (250–500 mg/day or 10g whole fruit/day). The only food with direct human trial data on fluoride excretion. The study limits are real — endemic fluorosis population, children, 18-day duration. But it’s the only data point we have that shows mobilization of deposited fluoride rather than just prevention of new absorption. That’s a meaningful distinction. See the full tamarind and pineal gland breakdown for mechanism details.
3. Vitamin K2 MK-7 (150 mcg) + D3 (3,000 IU) together. Activates the MGP pathway. D3 without K2 increases calcium absorption without directing it away from soft tissue — pairing them matters. Take them separately and you might be making the problem worse.
4. Boron (3 mg/day). Competes with fluoride in excretion pathways. Plausible mechanism, thin direct evidence in non-fluorosis populations. Low risk, reasonable rationale. See boron and pineal decalcification for the full evidence review.
5. Magnesium glycinate (300 mg/day). Regulates calcium metabolism and reduces ectopic calcification through multiple pathways. Broader evidence base than the others, less specific to the fluoride/pineal mechanism — but hard to argue against. See magnesium and the pineal gland for detail.
Five-ingredient protocol ranked by evidence strength. Fluoride elimination comes before any supplement — you can’t address calcification while loading the primary mineralizing agent.
Ready to Start?
If you’re at the point of acting on this, what’s actually inside the supplement matters. Most products in this category are dosed below clinical thresholds or rely on proprietary blends that obscure the real amounts.
Pineal XT is one of the formulations that aligns with the ingredients reviewed above — K2, D3, and supporting compounds formulated to support this process at doses that correspond to the research. It doesn’t promise structural reversal. Nothing honest should.
Pineal XT includes K2 and D3 aligned with the MGP pathway evidence. It doesn’t claim structural reversal — and neither should anything you consider.
Quick Verdict — Pineal XT
3.7/5
Formulated with K2, D3, and iodine — the ingredients most aligned with the MGP pathway and melatonin support reviewed in this article. Proprietary blend limits full dose transparency. 365-day guarantee makes it a low-risk trial.
The reversal mechanisms are real. Tamarind mobilizes fluoride from deposited tissue — human data supports that. K2 activates the body’s primary soft-tissue calcification inhibitor — the biochemistry is solid. Neither has been tested in a trial that measures pineal calcification as the actual endpoint. That gap is not a reason to dismiss the evidence. It’s a reason to set honest expectations.
Light calcification: the biological levers are probably working in more responsive substrate. Dense, decades-old deposits: stopping new progression is the realistic win, not full dissolution.
Here’s what I keep coming back to, though. Nobody asks the cost-of-inaction question. If calcification progresses uninterrupted for another 10 years — what does that cost in sleep quality, circadian function, melatonin production? That’s the real calculation. And it’s why the protocol is worth the effort even when the evidence is incomplete.
Start with fluoride elimination. A water filter and a different tube of toothpaste. That’s it.
Frequently Asked Questions
Can you reverse pineal gland calcification?
Partially, yes. Light-to-moderate calcification responds to a protocol combining K2 (MK-7), vitamin D3, tamarind extract, and fluoride elimination over 90–180 days. Severe, long-standing deposits may be structurally irreversible, but stopping further progression and restoring functional tissue is achievable.
Is pineal gland calcification permanent?
Not necessarily. Light calcification is more biologically reversible. Dense, decades-old fluorapatite deposits are harder to dissolve, but progression can be halted at any stage. The realistic goal for most people is partial reversal plus functional support, not complete dissolution.
What dissolves pineal gland calcification?
No substance is proven to fully dissolve established pineal calcification in humans. Tamarind extract increases urinary fluoride excretion (human trial data), and K2 activates MGP, the body's main soft-tissue calcification inhibitor. Together, they represent the strongest evidence-based approach available.
How long does it take to decalcify the pineal gland?
Sleep quality often improves in 30–60 days. A full protocol runs 90–180 days. Structural changes to calcification deposits, if they occur, likely require 12+ months — based on comparable K2 research in vascular tissue. Circadian consistency is the most reliable early progress signal.
Marcus Hale is an independent researcher and former clinical neuroscientist.
The content on PinealCode.com is for informational purposes only and does not
constitute medical advice.
Medical Disclaimer: The content on
PinealCode.com is for informational and educational purposes only. Nothing here
constitutes medical advice, diagnosis, or treatment. Always consult a qualified
healthcare provider before making changes to your health regimen.
Affiliate Disclosure: This article
contains affiliate links. Purchasing through these links may earn us a commission
at no extra cost to you.
Marcus Hale
Independent Researcher · Former Clinical Neuroscientist
I spent 12 years in clinical neurology before the questions got more interesting
than the answers. PinealCode is where I document what I find at the intersection
of brain science and consciousness.