How to Reverse Pineal Gland Calcification: A Realistic Protocol
Most articles about pineal gland calcification tell you to drink filtered water
and eat more greens. Then they stop.
That’s not a protocol. That’s a grocery list.
How to reverse pineal gland calcification is a legitimate question — and the
honest answer is: partially, for most people, with the right inputs over 90 to
180 days. How much reversal you get depends on how much calcification you’ve
accumulated, how long it’s been there, and what you’re willing to do
consistently.
This isn’t a detox cleanse. It’s a biochemical intervention with real mechanisms
and real limits. If you’ve already read about pineal gland calcification
symptoms and you’re here for
what comes next — this is that article.
Can You Reverse Pineal Gland Calcification?
Yes — but “reverse” is a marketing word. Biologically, what you’re doing is two
distinct things: dissolving recent deposits and preventing new ones from
forming.
Those are not the same goal. Conflating them is how most wellness content sets
people up for disappointment.
A 2018 review in Molecules by Tan, Xu, Zhou, and Reiter — four researchers
with serious neuroscience credentials — raised the possibility of “rejuvenating
the calcified pineal gland.” That phrase gets quoted everywhere. What gets left
out: it was a hypothesis in a review paper, not a finding from a clinical trial.
The authors were pointing toward a research direction. Not reporting a result.
Here’s what we actually know. Calcification builds with age — a 2023 cross-sectional analysis confirmed that calcification prevalence rises sharply and progressively through adulthood, with age, sex, and lipid metabolism among the principal associated factors. The accumulation
isn’t uniform: some people show significant calcification by their 30s, others
well into their 50s show only minor deposits. Light-to-moderate calcification,
the kind most people reading this have, appears more biologically reversible than
the dense, decades-old deposits you see on CT scans of elderly patients.
A 2026 study from Del Brutto et al. added a nuance worth sitting with: even with
measurable calcification, the remaining functional tissue may produce enough
melatonin to compensate. Stopping progression might matter more than we’ve
been told. Reversal might be less urgent than preventing further damage.
That’s uncomfortable for supplement companies. It’s useful for you.
Partial reversal is within reach for most people with light-to-moderate
calcification. Severe, long-standing deposits are a harder problem. Any article
promising to dissolve 20 years of buildup in 30 days is selling you something.
How Pineal Calcification Reversal Works (The Biology)
Here’s what’s actually happening inside the gland.
Calcium deposits in the pineal form primarily as hydroxyapatite — the same
mineral structure in bone. When fluoride is present in the tissue, it
substitutes into the hydroxyapatite lattice to form fluorapatite: a harder,
more stable compound that resists dissolution far more than regular calcium
deposits.
This is why eliminating fluoride is the first step in any rational protocol.
Not because it magically dissolves what’s already there — it doesn’t — but
because it stops the hardening process and removes the primary driver of new
formation.
I used to underestimate this part. I thought the fluoride-pineal connection was
overstated, mostly circulated in corners of the internet that also sell colloidal
silver. Then I actually read the Luke data. 296 mg/kg. That’s not trace exposure.
That’s preferential accumulation. The mechanism matters.
That data is vascular, not pineal. The extrapolation is mechanistically
reasonable — MGP operates systemically — but nobody has run a controlled trial
measuring MK-7’s effect on pineal tissue directly. We’re reasoning from first
principles. That’s worth saying plainly.
Tamarind works differently. A 2002 controlled human trial found that 10g of tamarind daily for 18 days increased urinary fluoride excretion by roughly 37% in human participants — from 3.5 to 4.8 mg per day (European Journal of Clinical Nutrition, Khandare et al.). A 2004 follow-up showed tamarind also
mobilizes fluoride already deposited in bone. Not just blocking new absorption.
Pulling out what’s already in there.
That’s the part most summaries miss.
Boron competes with fluoride at the cellular level, potentially limiting
fluoride’s ability to integrate into mineral deposits. The evidence is thinner
here — no human trial has directly measured boron’s effect on pineal fluoride
content. Plausible mechanism, honest disclaimer.
Three angles: stop the input, redirect the calcium, accelerate fluoride
excretion. That’s the logic behind what follows.
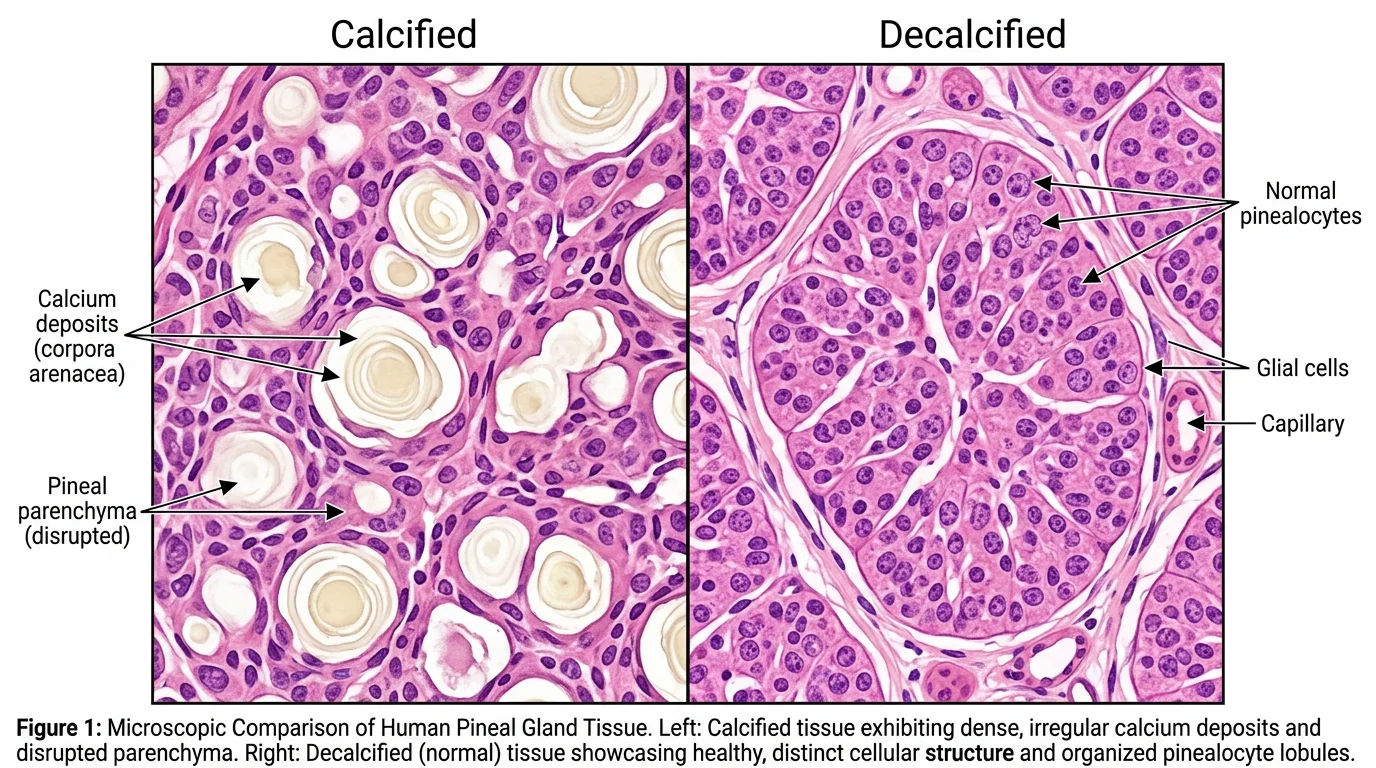
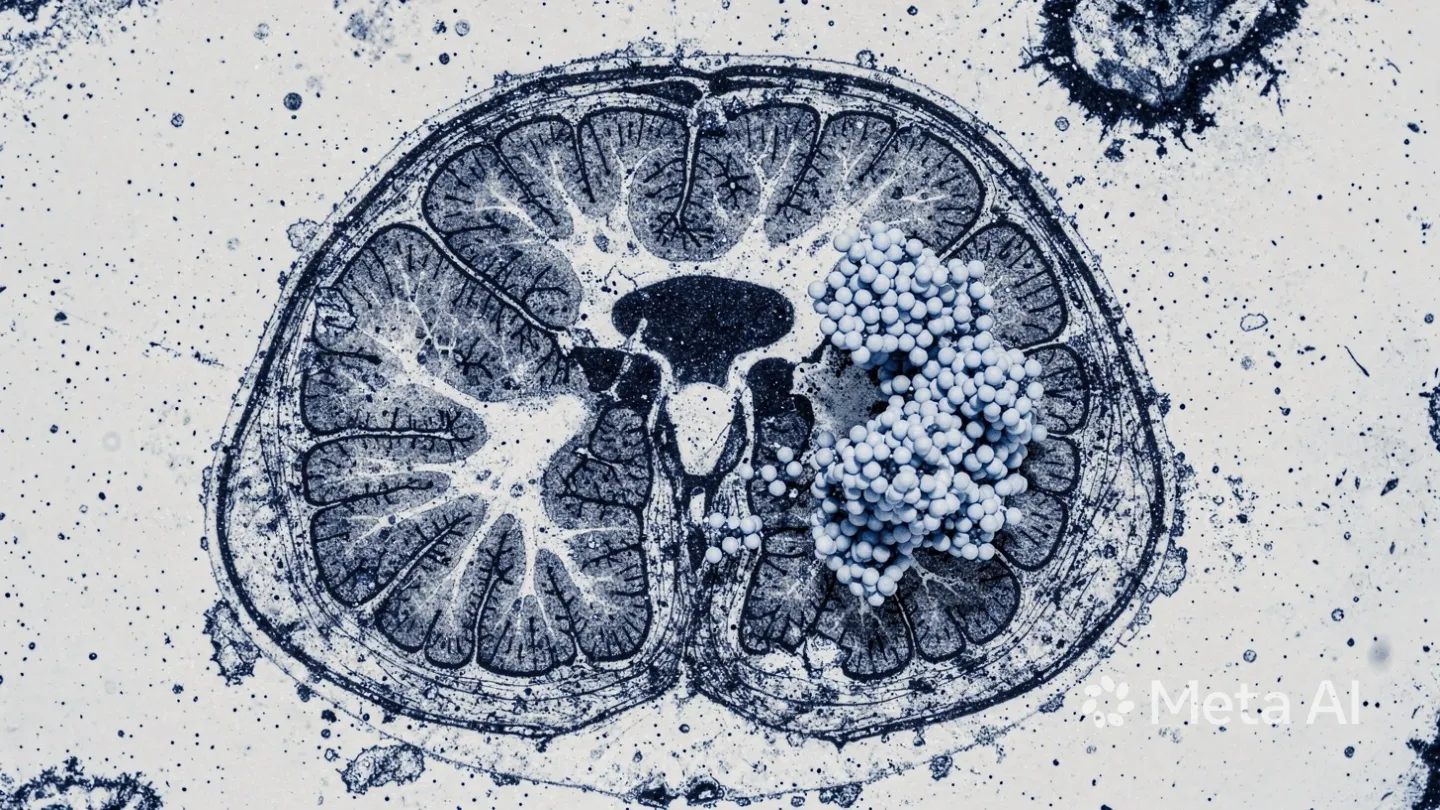
Calcified tissue (left): irregular calcium deposits disrupt cellular structure. Decalcified (right): distinct lobules with glial cells and capillaries intact
What Supplements Help Reverse Pineal Calcification?
The five compounds with the strongest mechanistic case, ordered by evidence
quality:
Supplement
Dose
Mechanism
Evidence Base
Expected Timeline
Vitamin K2 (MK-7)
100–200 mcg/day
Activates MGP → redirects calcium out of soft tissue
Vascular studies (extrapolated)
60–90 days
Vitamin D3
2,000–5,000 IU/day
Regulates calcium absorption; synergistic with K2
Strong for calcium regulation
30–60 days
Tamarind Extract
250–500 mg/day
Increases urinary fluoride excretion
Direct human trial (Khandare 2002)
20–60 days
Boron
3–6 mg/day
Fluoride antagonist at cellular level
Animal/mechanistic studies
60–90 days
Magnesium Glycinate
300–400 mg/day
Competes with calcium; reduces deposition
Established mechanism
Ongoing
A few things the table doesn’t capture:
On K2: Buy MK-7, not MK-4. They’re not interchangeable — MK-7 has a longer
half-life and better bioavailability for activating systemic MGP. Most cheap K2
products use MK-4. Check the label.
On D3: Don’t take D3 without K2. The concern — that D3 increases calcium
absorption, and without active MGP that calcium deposits in soft tissue — is
biologically sound even though direct human evidence at normal doses is limited.
This isn’t paranoia. It’s how these two nutrients work together by design.
On tamarind: The human studies used whole tamarind fruit (10g/day), not
extract. If you’re using an extract, 250–500 mg is the working dose, but no
trial validates that exact conversion. Whole tamarind stays closest to the
actual evidence.
K2 and D3 work synergistically — always take together for soft-tissue calcification protocols
Yes, there’s a supplement for that. There’s always a supplement for that. If you
want a formula combining several of these mechanisms, see our analysis of the
best supplement to decalcify the pineal gland
— or the detailed Pineal Guardian ingredient breakdown for a full examination of each botanical against the clinical evidence.
Quick Verdict — Pineal Guardian
3.95/5
Nine botanical ingredients including Tamarind (fluoride excretion), Chlorella (heavy metal chelation), and Ginkgo Biloba (cerebral circulation). Liquid drop delivery. Proprietary blend limits dose transparency, but the formula is well-researched for this category. 365-day guarantee.
Nobody gives you a timeline. That’s the most common complaint I see in forums —
people find protocols but no structure, no phasing, no honest answer to “when
will I know if this is working?”
Here’s the structure I’d follow if I were starting today.
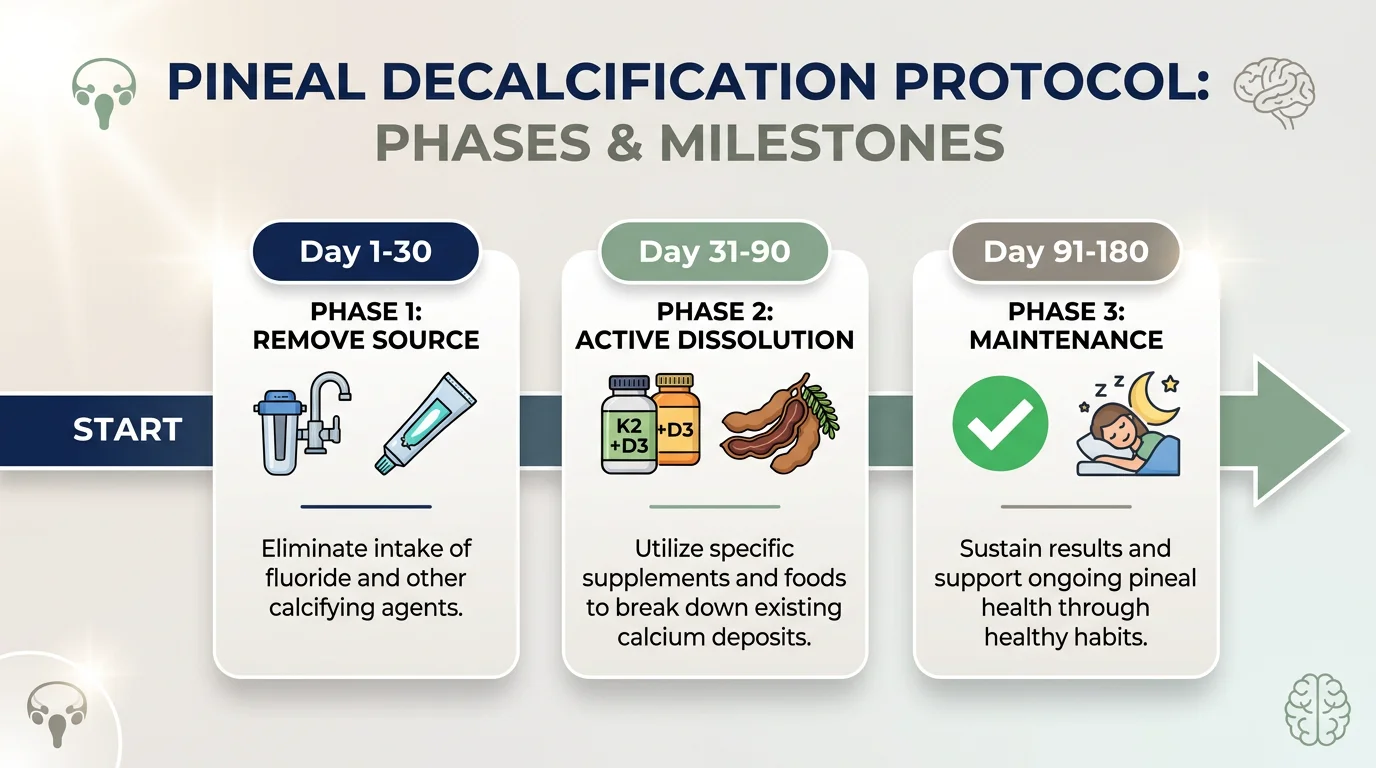
Phase 1 removes the source, Phase 2 targets existing deposits — don't skip the sequence
Phase 1: Remove the Source (Days 1–30)
Before adding anything, stop the input.
Switch to filtered water. Reverse osmosis or a Berkey-style filter removes
fluoride. Standard Brita filters do not. This matters because research confirms that fluoride concentrates in the pineal gland more than in brain tissue or bone, making it the soft-tissue site most vulnerable to ongoing fluoride accumulation.
Change your toothpaste. Fluoride-free options — hydroxyapatite-based or
plain — are easy to find.
Stop calcium carbonate supplements. Inorganic calcium drives soft-tissue
calcification. Switch to food sources or stop unless a doctor has directed
otherwise.
Start tamarind extract (250 mg/day) and magnesium glycinate (300 mg/day).
Low interaction risk. Direct mechanism. Good starting point.
Phase 1 isn’t dramatic. It’s removing what’s actively working against you.
Phase 2: Active Dissolution (Days 31–90)
With the source reduced, add the compounds that work on existing deposits.
K2 (MK-7, 150 mcg) + D3 (3,000 IU) — together, with a fatty meal. Both
are fat-soluble. Absorption without dietary fat is poor.
Boron (3 mg/day). Morning is fine.
Keep tamarind extract running. The 2004 Khandare data suggests the
fluoride-mobilizing effect builds over time.
Sleep in complete darkness. Endogenous melatonin requires it. If you want
to use your own sleep quality as a signal for whether this is working, you
need the signal to be clean.
By day 60, you should have some sense of whether sleep quality is shifting. That’s
the first and most reliable early marker — not cognitive clarity, not dreams.
Sleep depth first.
Phase 3: Maintenance & Assessment (Days 91–180)
At 90 days, pause and assess.
Continue K2+D3 at maintenance dose (100 mcg / 2,000 IU)
Calcification built over 20 years doesn’t dissolve in 90 days. Be honest with
yourself about that. If you’re not noticing anything by day 90, either the
protocol needs adjustment or the calcification is more extensive than a
supplement stack can address alone.
That’s a legitimate outcome. Not everything dissolves. Knowing that is also
useful information.
What Foods Help Decalcify the Pineal Gland?
Supplements move faster. But food-based support matters — and for some people,
it’s where they want to start.
Tamarind — the most evidence-backed option here. Soak 20g of whole
tamarind in 500ml of water overnight, drink in the morning. The studies used
extract; this is the food-form approximation. Indirect, but the underlying
mechanism is the same tartrate-based fluoride mobilization.
Soak 20g whole tamarind in 500ml water overnight — drink in the morning
Raw cacao — roughly 180mg of magnesium per 30g. Magnesium competes with
calcium at absorption sites; sustained high intake reduces ectopic calcium
deposition over time.
Chlorella or spirulina — both bind heavy metals in the gut and facilitate
excretion. Not pineal-specific. But reducing total metal load matters.
Garlic — selenium concentrates in the pineal gland more than most other
soft tissues. Organosulfur compounds in garlic also support phase II liver
detoxification, which feeds into overall metal clearance.
Apple cider vinegar — the acetic acid claim for dissolving calcium
deposits is overstated. Evidence is weak. Include it if you like the taste;
don’t count on it.
Not necessarily — but the answer depends on how severe it is and how long it’s
been there.
Light calcification, detectable on CT but not dramatically extensive, responds
more readily to the mechanisms above. The K2/MGP pathway works against newer,
less crystallized deposits. Tamarind addresses the fluoride component that makes
deposits resistant to dissolution.
Dense, decades-old calcification is a different problem. Full stop.
Once fluorapatite has fully crystallized over many years, the biological
processes that might reverse it face a harder target. The vascular calcification
literature — which has more direct human data than pineal research does — shows
modest but real reductions in calcification scores with K2 intervention over 1–2
years. A 2023 randomized controlled trial (Trevasc-HDK) showed MK-7 reduced the
inactive dp-ucMGP biomarker by 40–45%, even when calcification scores themselves
didn’t change dramatically in the study window.
Biomarker improvement without immediate structural change is still something.
The machinery is working again. The deposit takes longer to shift.
If you’re 65 with extensive calcification on imaging, this protocol may slow
progression and support remaining functional tissue. It probably won’t dissolve
what’s been there since your 40s. That’s still worth doing — not because it
promises reversal, but because stopping forward momentum is its own outcome.
What This Means for You
Here’s where the evidence actually lands.
What the research supports:
Fluoride accumulates in the pineal at concentrations far beyond other soft
tissues — peer-reviewed, undisputed
K2 (MK-7) activates MGP, the primary inhibitor of soft-tissue calcification
Tamarind increases urinary fluoride excretion in humans — direct trial data,
n=18, modest but real
Calcification correlates with worse sleep and lower melatonin in recent
imaging studies
What the research does not support:
A controlled human trial measuring reversal of pineal calcification by any
intervention does not exist
The tamarind extract dose that replicates the 10g whole-food studies is
unvalidated
Boron’s fluoride-antagonism in pineal tissue is plausible mechanistically,
not proven clinically
This is a protocol built on the best available evidence, with honest
acknowledgment of what that evidence can and can’t prove. If a site tells you
otherwise, they’re selling harder than they’re thinking.
Start with Phase 1. Filter your water, change your toothpaste, add magnesium.
Those steps cost almost nothing and remove the active drivers of the problem.
Everything else builds from there.
Frequently Asked Questions
Can you reverse pineal gland calcification?
Partially yes. Light-to-moderate calcification responds to a protocol combining K2 (MK-7), D3, tamarind extract, and fluoride elimination over 90–180 days. Severe or decades-old calcification may be irreversible structurally, but progression can be halted and remaining tissue supported.
How long does it take to decalcify the pineal gland?
Expect 60–90 days to notice improvements in sleep quality as the first signal. A full protocol runs 180 days. Calcification built over 20+ years will not resolve in 30 days — use sleep depth and circadian consistency as your primary progress metrics.
What supplements help reverse pineal calcification?
Vitamin K2 (MK-7, 150 mcg), Vitamin D3 (3,000 IU), Tamarind extract (250–500 mg), Boron (3 mg), and Magnesium glycinate (300 mg). Always take K2 with D3 — the two work together via the MGP calcium-redirection pathway.
Is pineal gland calcification permanent?
Not always. Light-to-moderate calcification can be partially reversed with the K2+tamarind+fluoride elimination protocol. Dense, long-standing deposits may not fully dissolve, but stopping further progression and supporting remaining melatonin-producing tissue is achievable at any stage.
Does fluoride cause pineal gland calcification?
Yes — fluoride concentrates in the pineal gland at levels far higher than any other soft tissue, bonding with calcium to form fluorapatite crystals that are harder to dissolve than regular hydroxyapatite. Removing fluoride from your water and toothpaste is the first step in any reversal protocol.
Marcus Hale is an independent researcher and former clinical neuroscientist
based in Austin, Texas. The content on PinealCode.com is for informational
purposes only and does not constitute medical advice. Consult a qualified
healthcare provider before starting any supplement protocol.
Medical Disclaimer: The content on
PinealCode.com is for informational and educational purposes only. Nothing here
constitutes medical advice, diagnosis, or treatment. Always consult a qualified
healthcare provider before making changes to your health regimen.
Marcus Hale
Independent Researcher · Former Clinical Neuroscientist
I spent 12 years in clinical neurology before the questions got more interesting
than the answers. PinealCode is where I document what I find at the intersection
of brain science and consciousness.