
8 min read
Iodine Pineal Gland: The NIS Mechanism 4M Sites Got Wrong
4 million results claim iodine decalcifies the pineal gland. The NIS mechanism is real — the extrapolation isn't. Here's where the evidence...
April 14, 2026
Read →
“Bulky pineal gland with rim calcification.” If those words appeared on your MRI report, here’s what they actually mean. Your first instinct to Google it at midnight is understandable. It’s also probably unnecessary.
Radiology reports are written for other radiologists. Not for you. The language is precise, technical, and almost designed to sound alarming to anyone without a medical degree. “Bulky.” “Calcification.” “Rim pattern.” Each of these words has a specific meaning that’s far less dramatic than it sounds.
I spent over a decade in clinical neuroscience research. I’ve seen how these reports get handed to patients with zero context, zero explanation, and zero acknowledgment that the person holding the paper is now quietly panicking. That’s a failure of communication, not a sign something is wrong with your brain.
Here’s what the research actually shows. And what it doesn’t.
It means the pineal gland appears slightly larger than average on imaging, with calcium deposits concentrated around its outer edge rather than distributed throughout its interior.
Let’s break that down.
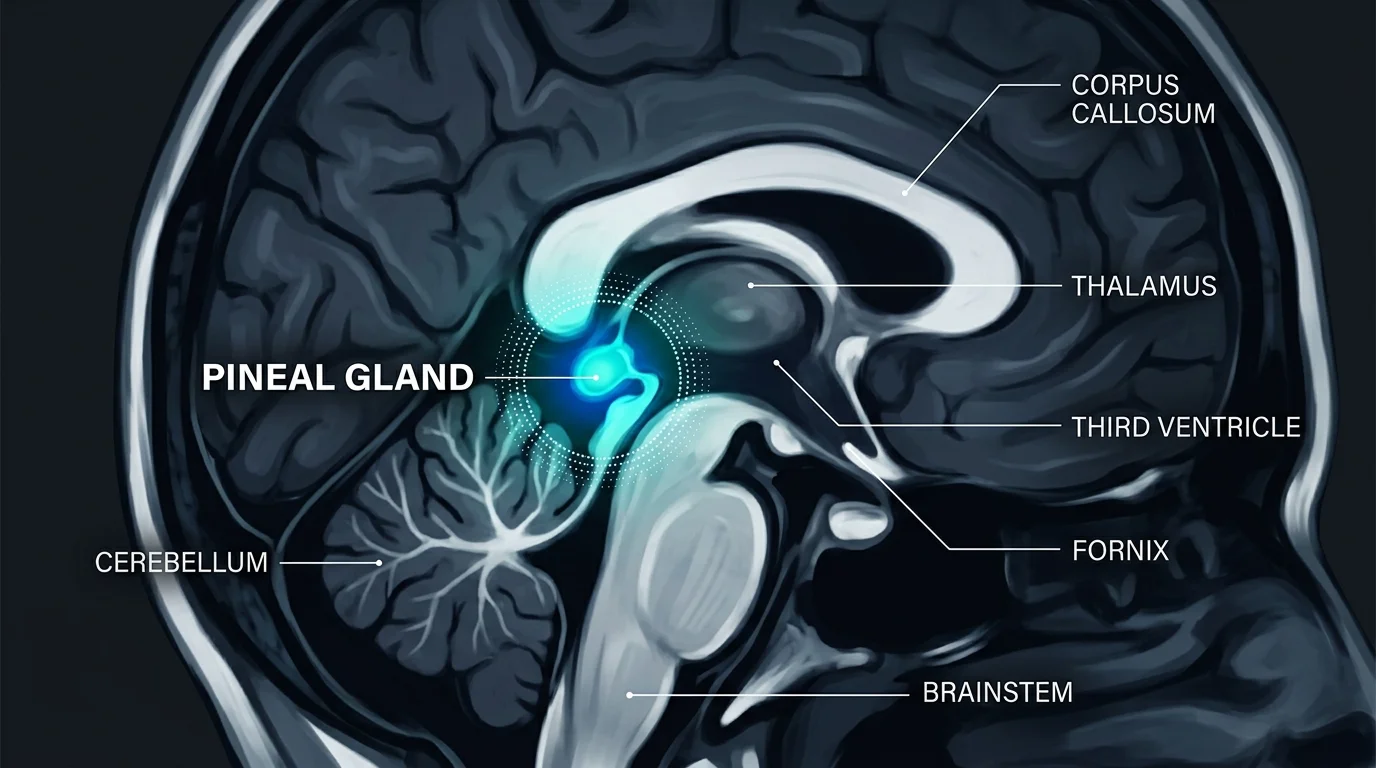
“Bulky” is radiologist shorthand for a gland measuring above roughly 1 cm³ in volume. There’s no universally agreed threshold written into formal guidelines, which itself tells you something about how imprecise this territory is. The pineal gland is typically the size of a pea. When it reads as “bulky,” it’s usually because a small fluid-filled cyst inside the gland is pushing its walls outward.
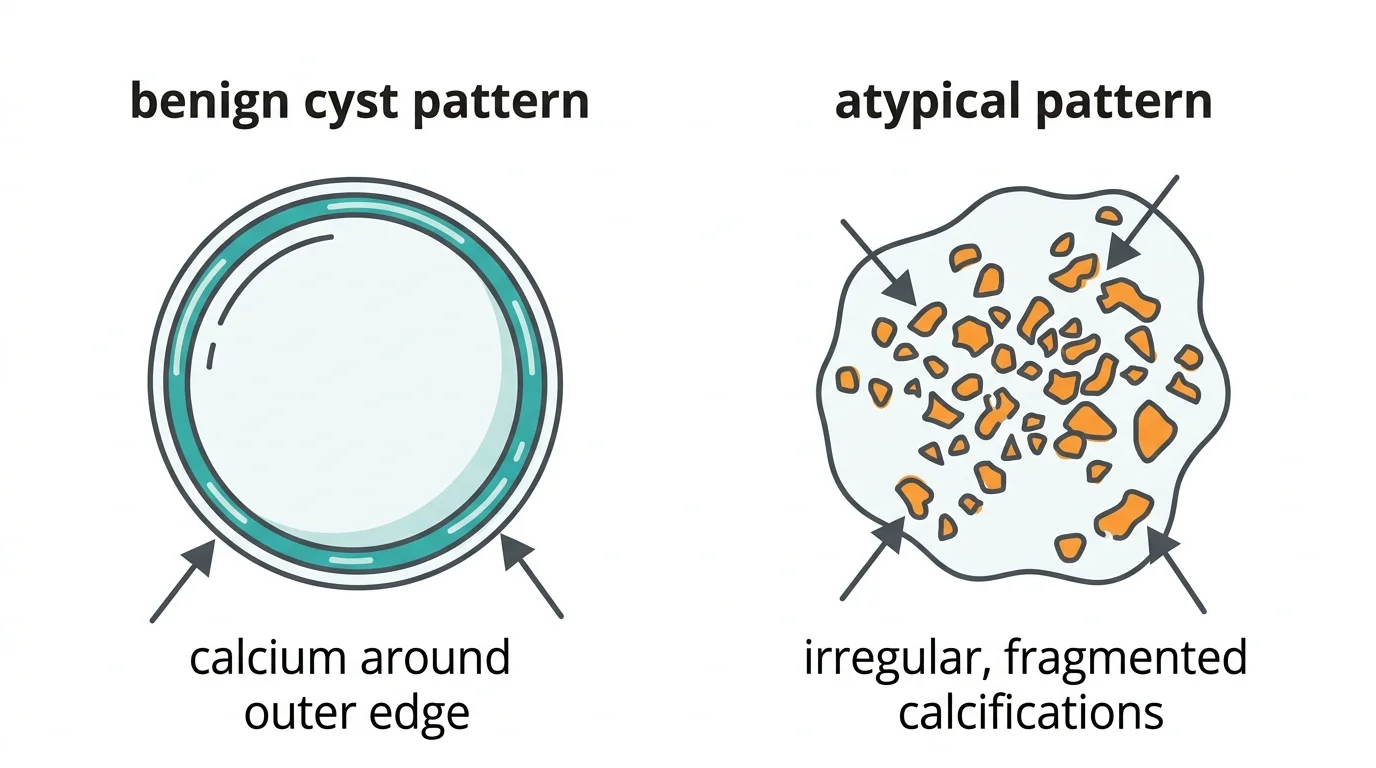
“Rim calcification” describes where the calcium is sitting. Not diffusely scattered through the tissue. Not clumped into a dense nodule at the center. Around the perimeter. The rim. This peripheral pattern matters because it’s strongly associated with benign cysts, not tumors.
The pineal gland shows up in Descartes’ philosophy, religious iconography, and an improbable number of tattoo designs. It does not, as a rule, show up in routine patient education — which is exactly why finding it on a report feels like discovering something classified when it’s actually one of the most commonly observed structures in adult neuroimaging. For a broader look at what pineal gland calcification symptoms actually look like, that article covers the functional side.
A bulky pineal gland with rim calcification on MRI most commonly represents a benign pineal cyst with calcium deposits along its outer wall — a finding present in up to 40–60% of adults depending on imaging modality, according to population studies including a 2023 systematic review by Belay and Worku published in Systematic Reviews.
That number is not a typo. This is common. Shockingly common, given how rarely anyone mentions it until a report lands in your hands.
In most cases, no. Rim calcification is an incidental, benign finding. It showed up on the scan by accident, while the machine was looking for something else entirely, and it’s almost certainly not causing your symptoms.
The pattern matters. A lot.
Peripheral calcification — the rim pattern — is what you see when a cyst develops a calcified wall over time. Think of it as a scar. Diffuse calcification throughout the gland tissue is normal with aging. The pattern that actually raises flags is “exploded” or scattered calcification, where deposits appear displaced away from the center. That pattern is associated with tumors pushing the calcification outward from inside.
Rim calcification does not look like that.
When does it warrant more attention? The cystic component needs to be large, above 15 mm. Or there’s evidence of compression on surrounding structures like the cerebral aqueduct. Or you have neurological symptoms: persistent headaches, double vision, difficulty with upward gaze.
Absent those? Most radiologists file it under “incidental finding” and recommend follow-up imaging.
Pineal calcification starts as early as age two. By adulthood, this is simply what the gland does. Hydroxyapatite, the same mineral that makes bone hard, slowly deposits in the pineal tissue over decades. It’s not pathological. It’s biology.
A 2016 study by Beker-Acay and colleagues tracking 167 patients across age groups found that calcification increases progressively through middle age. The gland doesn’t fight it. It calcifies, slowly, as part of normal aging, the way joints stiffen and arteries lose elasticity.
Environmental factors — including fluoride exposure — are documented to accelerate this process. The full mechanism is covered in the fluoride and pineal gland breakdown.
When the gland reads as “bulky,” it’s usually because aging calcification is happening alongside something else.
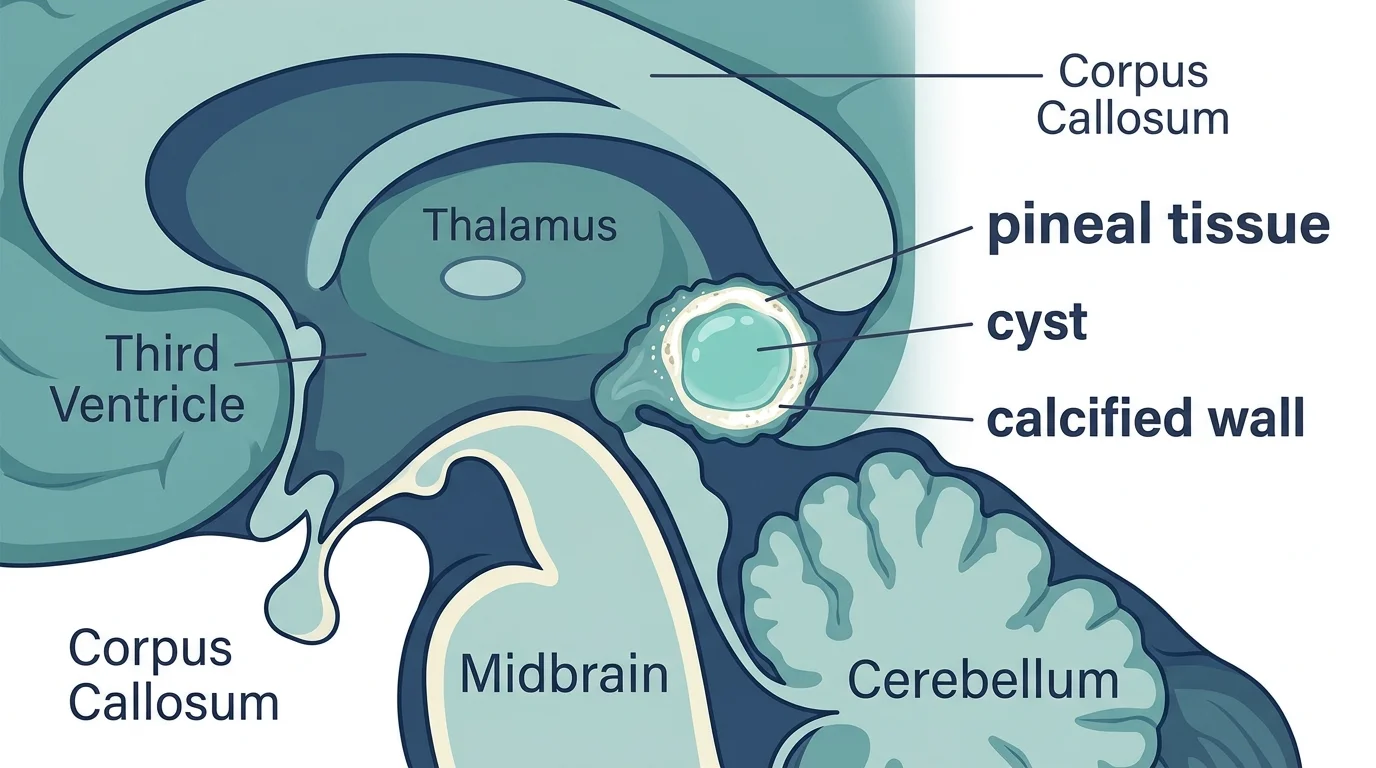
Pineal cysts are small fluid-filled structures within the gland. In routine MRI they appear in roughly 1–4% of the population, but that number climbs dramatically with higher-resolution imaging. A 2007 study in the American Journal of Neuroradiology found that when high-resolution protocols were used, prevalence approached the 25–40% range seen in autopsy series. Most cysts just aren’t visible on standard scans.
When a pineal cyst develops a calcified wall, you get exactly the “bulky pineal gland with rim calcification” pattern described in radiology reports.
What happens to these cysts over time is mostly good news. Al-Holou and colleagues (2011, Journal of Neurosurgery) followed 151 patients with pineal cysts over a mean of 3.4 years: 82% were completely stable, 15% actually shrank, and only 2.6% showed any growth. None required emergency surgery.
Nevins and colleagues (2016, World Neurosurgery) reviewed over 42,000 MRIs and found that only 6% of incidental pineal cysts changed in size during follow-up. Their conclusion: a single follow-up MRI at 12 months is sufficient for asymptomatic cases.
One scan. Twelve months. Then, usually, nothing more.
Pineal region tumors exist. They account for less than 1% of all brain tumors in adults, per Solomou’s 2017 review in Rare Tumors, and around 3–8% in pediatric populations. Rare. But worth understanding so you know what the red flags actually look like.
I’ll be honest: when I first started encountering the distinction between rim and “exploded” calcification patterns in clinical settings, I filed it under radiologist trivia — pattern recognition for people who read scans all day. I came around. The pattern genuinely matters for deciding how aggressively you pursue follow-up imaging.
Pineocytomas are the slow-growing, low-grade variant. They tend to appear in adults around age 38, behave like benign lesions, and have good long-term outcomes. Pineoblastomas are aggressive, predominantly in younger patients, and require very different management.
The distinguishing feature on imaging: peripheral rim calcification points toward cyst. Scattered calcification with displaced fragments surrounding a mass is more suspicious for tumor. Heterogeneous enhancement after contrast, irregular borders, surrounding edema — those are the features that prompt urgent neurosurgical referral.
Fakhran and Escott (2008, AJNR) demonstrated that when strict criteria are applied on contrast-enhanced MRI — no nodular enhancement, wall thickness under 2 mm, no marginal lobulation — the ability to exclude tumor is quite reliable.
The problem: not every MRI is done with contrast. Not every protocol is optimized for pineal evaluation. Which is why the follow-up recommendation exists.
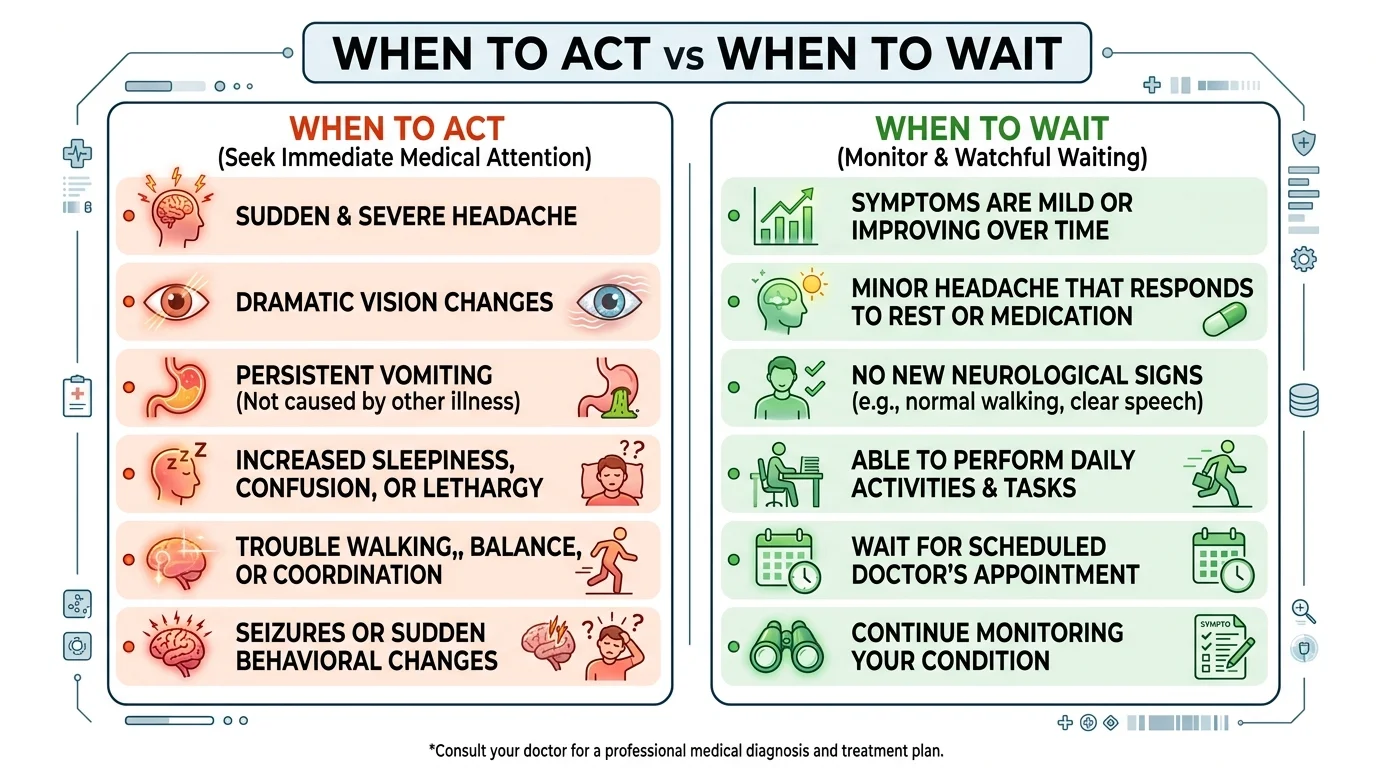
Probably not. But “watchful waiting” is not the same as ignoring it.
If the finding was incidental, you’re asymptomatic, and the report doesn’t describe any concerning features, your next step is a conversation with the ordering physician — not a neurosurgery consult. Most will recommend a follow-up MRI at 6–12 months to confirm stability.
The scenarios that justify moving faster:
Persistent headaches that are new in character or worse in the morning. Morning headaches from elevated intracranial pressure have a specific quality: dull, positional, better after standing up. Different from tension headaches. If that’s what you’ve been experiencing, say so explicitly.
Visual disturbances. The pineal region sits near structures controlling eye movement. Diplopia (double vision) or Parinaud syndrome (difficulty looking upward) are the classic compression findings. Either one warrants an expedited neurology appointment.
Hydrocephalus on the imaging report. If you see that, stop reading this article and call your doctor today.
None of those? Then this finding is almost certainly not what’s causing whatever brought you to the MRI in the first place.
One more thing the pineal health community tends to skip over: for most people who discover calcification incidentally, the calcification is not the problem you came in for. The headache, the sleep issue, whatever drove you to imaging — that’s probably unrelated. Don’t let the report redirect your attention away from the original symptom.
These terms describe different things that often occur together.
Calcification is the process: mineral deposits accumulating within or around the gland. Bulky describes the result: a gland that measures larger than typical on imaging.
Related, but not equivalent. A gland can be calcified without being bulky. A bulky gland usually has some form of calcification, often because a cyst is expanding its walls while calcium accumulates along those same walls.
The cyst provides the bulk. The calcification defines the rim. Together they produce the phrasing that ends up on your report.
What the research still doesn’t tell us is whether the specific combination — bulky plus rim — changes long-term outcomes compared to either finding alone. Studies on pineal cyst natural history generally don’t stratify by calcification pattern. That’s a real gap, and anyone telling you otherwise is filling in blanks the data doesn’t support.
If you’re interested in the underlying mineral chemistry of pineal calcification — how the hydroxyapatite crystals form and what’s been found inside them — pineal gland crystals covers the science in detail.
A bulky pineal gland with rim calcification is, in most adults, a benign incidental finding. It probably represents a pineal cyst with a calcified wall, a structure that has been sitting there quietly, doing nothing, possibly for years before this MRI happened to catch it.
These findings are common. They tend to stay stable on follow-up. The overwhelming majority of people who see this on a report will never need anything done about it.
That doesn’t mean dismiss it. It means put it in the right frame. Ask your doctor specifically: Does this finding require follow-up imaging? Are there any features on my report that concern you? Should I see a neurologist?
If you have no symptoms and the report doesn’t flag anything atypical, the answer to “what do I do now” is: a follow-up MRI in a year, and stop Googling at midnight.
If you’re curious about lifestyle factors that influence pineal health over the long term — including whether calcification can be slowed or partially addressed — how to decalcify the pineal gland naturally is a reasonable next read. Just don’t confuse general wellness optimization with the clinical management of what showed up on your scan.
Start with your doctor. Start there.
Marcus Hale is an independent researcher and former clinical neuroscientist. The content on PinealCode.com is for informational purposes only and does not constitute medical advice.
4 million results claim iodine decalcifies the pineal gland. The NIS mechanism is real — the extrapolation isn't. Here's where the evidence...
C60 binds up to 6 electrons at once — no other antioxidant works this way. Whether it protects your pineal from calcification: the honest...

WiFi and pineal calcification — what the science actually shows. Volkow 2011, Baconnier 2002 crystals, calcium channels. Honest analysis,...
Marcus Hale
Independent Researcher · Former Clinical Neuroscientist
I spent 12 years in clinical neurology before the questions got more interesting than the answers. PinealCode is where I document what I find at the intersection of brain science and consciousness.