You wake at 3 a.m. again. Same time, every night. By 7 a.m., your eyes are cement. Coffee doesn’t touch it. Neither does the additional sleep you’re chasing on weekends. Your doctor ran the standard panel — thyroid, iron, B12. Everything came back normal. They said it was stress. They said sleep hygiene. They didn’t check one small structure in the center of your brain that controls the very hormone that makes sleep possible.
It’s called the pineal gland. And something specific may be happening inside it.
The term pineal gland calcification symptoms isn’t in most medical textbooks because most doctors don’t systematically image for it. But once you start looking at the research — the prevalence data, the sleep studies, the melatonin correlations — a pattern emerges. Calcium deposits accumulating in pineal tissue. Melatonin production declining. Sleep integrity collapsing. Brain fog that feels like static.
This isn’t about mysticism. This is about a measurable physiological condition with documented neurochemical consequences that nobody checked for in your case.
What Is Pineal Gland Calcification?
The pineal gland is a pea-sized endocrine organ located in the geometric center of the brain. Its primary function: synthesize melatonin, the hormone that regulates your circadian rhythm and sleep-wake cycle.
Calcification is the accumulation of calcium phosphate deposits in pineal tissue over time. It’s not an infection. It’s not inflammation. It’s mineralization — the same process that hardens bones, happening inside this delicate gland.
A 2023 meta-analysis found a pooled prevalence of 61.65% for pineal gland calcification across imaging studies, with ranges from 35% to 76% depending on population and methodology — making it the statistical majority among adults. A Turkish study of 12,000 healthy individuals found that 71.6% showed intracranial calcifications, with the pineal gland being the most common site.
Calcification can begin as early as age 5. It increases steadily with age.
That number — 71.6% — stopped me when I first encountered it. I’d expected a condition that affected a minority. Something exotic. Instead it’s the statistical majority. Most adults walking around have calcium deposits in this gland and have never been told, because nobody checked.
Normal prevalence doesn’t mean normal consequences. Just because 71.6% of people have it doesn’t mean 71.6% are unaffected. Distribution matters. Degree matters. Whether the calcification is incidental or functionally relevant matters. The research suggests it does matter — and the functional relevance scales with extent.
Symptoms of a Calcified Pineal Gland: What Research Actually Shows
Sleep Problems: The Strongest Connection
The data here is the most direct.
Calcium deposits reduce the number of functional pinealocytes — the cells that actually produce melatonin. Less melatonin means a disrupted circadian rhythm. This is documented in literature dating back to a 1999 Nature paper on pineal function and aging.
Melatonin production is directly tied to the volume of non-calcified pineal tissue. More calcification, less viable tissue. Less viable tissue, less melatonin. Less melatonin, worse sleep architecture.
Specific symptoms: difficulty falling asleep despite exhaustion. Frequent waking between 2 and 4 a.m. — the peak window for melatonin secretion. Sleep that feels non-restorative even when duration is adequate. Excessive daytime fatigue disproportionate to activity level.
Honest caveat: a 2026 study notes that evidence for non-apnea sleep symptoms remains inconclusive for mild-to-moderate calcification. The strongest data exists for advanced cases. Mild calcification puts you in the territory of correlation and plausibility, not yet proof.
Brain Fog and Cognitive Effects
Melatonin deficiency leads to increased oxidative stress in the brain (PMC6017004, 2018). Oxidative stress damages neurons. Damaged neurons don’t process information cleanly.
But that’s advanced pathology. The leap from mild calcification to cognitive decline isn’t a straight line.
What people commonly report: difficulty concentrating on a single task. Word retrieval problems. Mental slowness — that sensation of operating at 60% clock speed. A persistent fog that lifts slightly with sleep but never fully clears.
The research suggests a plausible mechanism. The association with advanced cognitive disease is documented. The clinical protocol connecting mild calcification to these everyday symptoms? Still being established.
Mood, Hormones, and Circadian Disruption
MRI research shows that reduced pineal volume is associated with major depressive disorder and bipolar disorder, with pineal abnormalities correlating specifically with symptoms in non-melancholic MDD subtypes — including loss of interest and emotional instability. Abnormal melatonin secretion patterns have been demonstrated in affective disorders. Melatonin isn’t just about sleep — it’s a chronobiotic hormone that regulates mood stability through circadian entrainment.
Melatonin also functions as a gonadal inhibitor. Impaired pineal function in children has been associated with early pubertal onset via reduced suppression of gonadotropin-releasing hormone.
Mood symptoms: irritability, emotional instability, seasonal mood shifts that don’t align with your environmental context, difficulty regulating emotional responses to minor stressors.
These aren’t new to you. They’re the texture of your daily life that you’ve stopped mentioning to doctors because the answer is always the same. Some practitioners working on circadian regulation through meditation report the pressure sensation between the eyebrows as an early indicator of improving prefrontal-thalamic connectivity — the same network disrupted by melatonin dysregulation.
How Do You Know If Your Pineal Gland Is Calcified?
Imaging is the only definitive answer.
CT scan is most sensitive. MRI can detect it but is less reliable for fine calcifications. No blood test exists for pineal calcification. No saliva test. No biomarker panel.
Calcification is almost always an incidental finding. Radiologists identify it when they’re looking for something else — a tumor, a stroke, hemorrhage. They note it in the report. Most clinicians don’t order imaging specifically to assess pineal status.
A symptom cluster — sleep disruption plus fatigue plus brain fog — is suggestive. Not diagnostic. It’s the reason to ask for imaging.
Age is a rough proxy. Above 30, probability increases significantly. Above 50, assume some degree of calcification exists.
B12 deficiency and iron deficiency create cognitive symptoms indistinguishable from melatonin-related dysfunction.
Sleep apnea causes the exact fatigue and poor sleep quality described here, through oxygen disruption rather than hormonal.
Chronic stress dysregulates cortisol and can mimic everything on this list.
Calcification rarely acts alone. You almost never have a single isolated cause. But it may be the single factor nobody investigated in your case, because the standard protocol doesn’t include imaging for it.
WiFi and EMF exposure are frequently cited in this space as a cause of calcification — but the evidence doesn’t support that claim at this point. The actual research on EMF and the pineal gland shows measurable biological effects from radiofrequency radiation, but no direct link to calcification rates in humans. The causes with documented evidence are fluoride and aging, not your router.
The thyroid panel matters. The B12 test matters. The sleep study might matter. Get those eliminated from the equation first. Then, if the answers are still incomplete, ask about imaging.
What Science Still Doesn’t Know
There is no proven causal chain from mild calcification to specific symptom clusters.
No established threshold exists: how much calcification causes symptoms? 5%? 50% of pineal tissue compromised? The research doesn’t say. Nobody has drawn that line yet, and anyone claiming to know the number is working from inference, not data.
No randomized controlled trial has tested decalcification interventions and measured symptom improvement. That work hasn’t been done.
The 2026 literature still lists non-apnea sleep symptoms as inconclusive for mild-to-moderate cases.
Here’s my honest position on the “reversal” conversation — and it cuts against the grain of most content in this space: I think the focus on reversing calcification is largely misplaced. Calcium deposits that have formed don’t dissolve easily, and the research on interventions that might reverse them is thin to nonexistent. The more realistic and better-supported goal is preserving the tissue that still functions. Protecting what remains. Slowing progression. That’s less exciting to write about — but the practices with the strongest evidence for pineal support are covered in how to open your third eye: meditation, breathwork, and light exposure. Those have real data. The decalcification mythology mostly doesn’t.
The correlation is real. The mechanism is plausible. The clinical protocol doesn’t exist yet. That’s the honest position.
What to Do Next
Start with sleep. Not supplements. Not imaging. Sleep.
Fix circadian rhythm before anything else. Light exposure within 30 minutes of waking. Darkness after sunset. Consistent sleep-wake times. Melatonin can’t be replaced by supplementation if you’re sending contradictory circadian signals through light exposure every evening.
Reduce fluoride. Fluoride has documented affinity for calcifying tissue, including pineal tissue. Consider water filtration. The detailed breakdown is in fluoride and the pineal gland.
Nutritional support: magnesium (calcium regulation), vitamin K2 (directs calcium to the right places), iodine (thyroid and pineal function). Pineal Guardian is formulated specifically around these compounds as a foundation — not a cure, a foundation. I’ve reviewed every ingredient and the evidence behind each dose in the Pineal Guardian review.
See a doctor. Not to confirm your suspicions about calcification — to rule out thyroid dysfunction, B12 deficiency, iron deficiency, and sleep apnea. These are testable. These are treatable. Eliminate them from the equation first. If your doctor is open to it, ask for a CT scan framed around the sleep and cognitive symptoms. Don’t lead with “I think my pineal gland is calcified.” Lead with the symptoms. Let the imaging find what it finds.
Frequently Asked Questions
What are the symptoms of a calcified pineal gland?
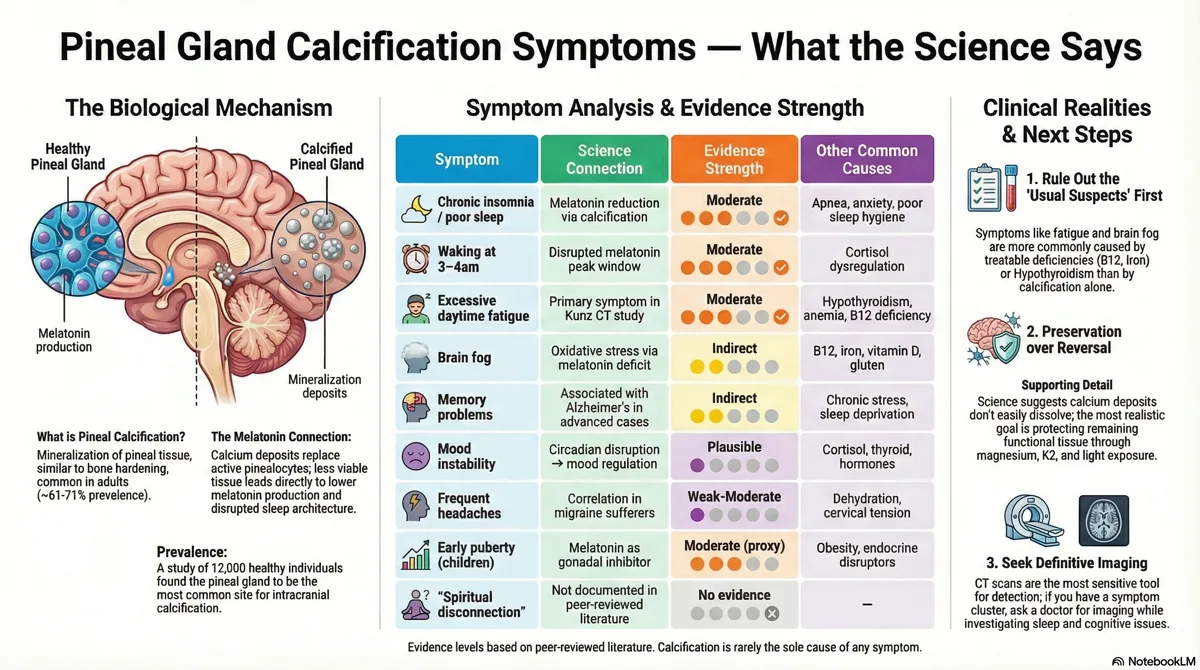
Sleep disruption — insomnia, frequent waking (especially 2–4am), non-restorative sleep. Excessive daytime fatigue. Brain fog. Difficulty concentrating. Mood instability. Memory problems. Some report frequent headaches or seasonal mood shifts. The symptom profile depends on degree of calcification and individual sensitivity.
Can a calcified pineal gland cause sleep problems?
Yes — the research supports this connection. Calcification reduces melatonin-producing pinealocytes. Less melatonin means disrupted circadian rhythm. The Kunz study directly correlated CT-graded calcification with sleep disturbance, with daytime fatigue as the primary symptom. Sleep problems have multiple causes — calcification may be contributing, not necessarily the only cause.
How do I know if my pineal gland is calcified?
Imaging is the only definitive answer. A CT scan will show calcification if present. You can't determine this through symptoms alone or blood tests. If you have the symptom cluster — sleep disruption, fatigue, brain fog — ask your doctor for imaging when investigating these issues.
Does pineal gland calcification affect melatonin?
Yes. Calcification reduces the number of pinealocytes capable of synthesizing melatonin. Less viable tissue means less melatonin, which disrupts circadian rhythm and sleep quality. The degree of reduction correlates with the extent of calcification.
Can pineal gland calcification cause headaches?
There's a documented correlation between pineal calcification and migraine frequency in some populations. The mechanism isn't fully established — it may involve circadian disruption, melatonin's neuroprotective role, or physical effects on adjacent structures. Evidence for headaches is weaker than for sleep symptoms.
Is pineal gland calcification reversible?
Calcium deposits once formed don't spontaneously dissolve. Decalcification strategies — reducing fluoride exposure, supporting calcium regulation through K2 and magnesium, optimizing circadian rhythm — can potentially slow progression and support remaining healthy tissue. Reversal isn't guaranteed. Functional improvement through supporting what remains is the more realistic and better-documented goal.
Marcus Hale is an independent researcher and former clinical neuroscientist. The content on PinealCode.com is for informational purposes only and does not constitute medical advice.
Medical Disclaimer: The content on
PinealCode.com is for informational and educational purposes only. Nothing here
constitutes medical advice, diagnosis, or treatment. Always consult a qualified
healthcare provider before making changes to your health regimen.
Affiliate Disclosure: This article
contains affiliate links. Purchasing through these links may earn us a commission
at no extra cost to you.
Marcus Hale
Independent Researcher · Former Clinical Neuroscientist
I spent 12 years in clinical neurology before the questions got more interesting
than the answers. PinealCode is where I document what I find at the intersection
of brain science and consciousness.