How to Know If Pineal Gland Is Calcified: 61.65% Have It
By Marcus Hale·
Most Adults Have a Calcified Pineal Gland — Here’s How to Know If You’re One of Them
Here’s the uncomfortable truth about pineal gland calcification: most adults already have it.
A 2023 systematic review published in Systematic Reviews (BioMed Central) found a pooled prevalence of 61.65% in the adult population. That’s not a fringe finding — that’s the majority of people reading this sentence. Which raises an obvious question: if calcification is that common, why does it matter? And if you’ve been wondering how to know if your pineal gland is calcified, the honest answer has two parts.
Part one: there are symptoms associated with calcification — sleep disruption, mood shifts, cognitive fog — backed by varying levels of evidence. Part two: none of those symptoms confirm calcification. The only thing that confirms it is medical imaging.
What follows is a breakdown of the 7 most reported signs, their actual evidence ratings, who’s at highest risk, and what a real diagnosis looks like. No mysticism. No invented studies. Just what we know, what we suspect, and where the research stops.
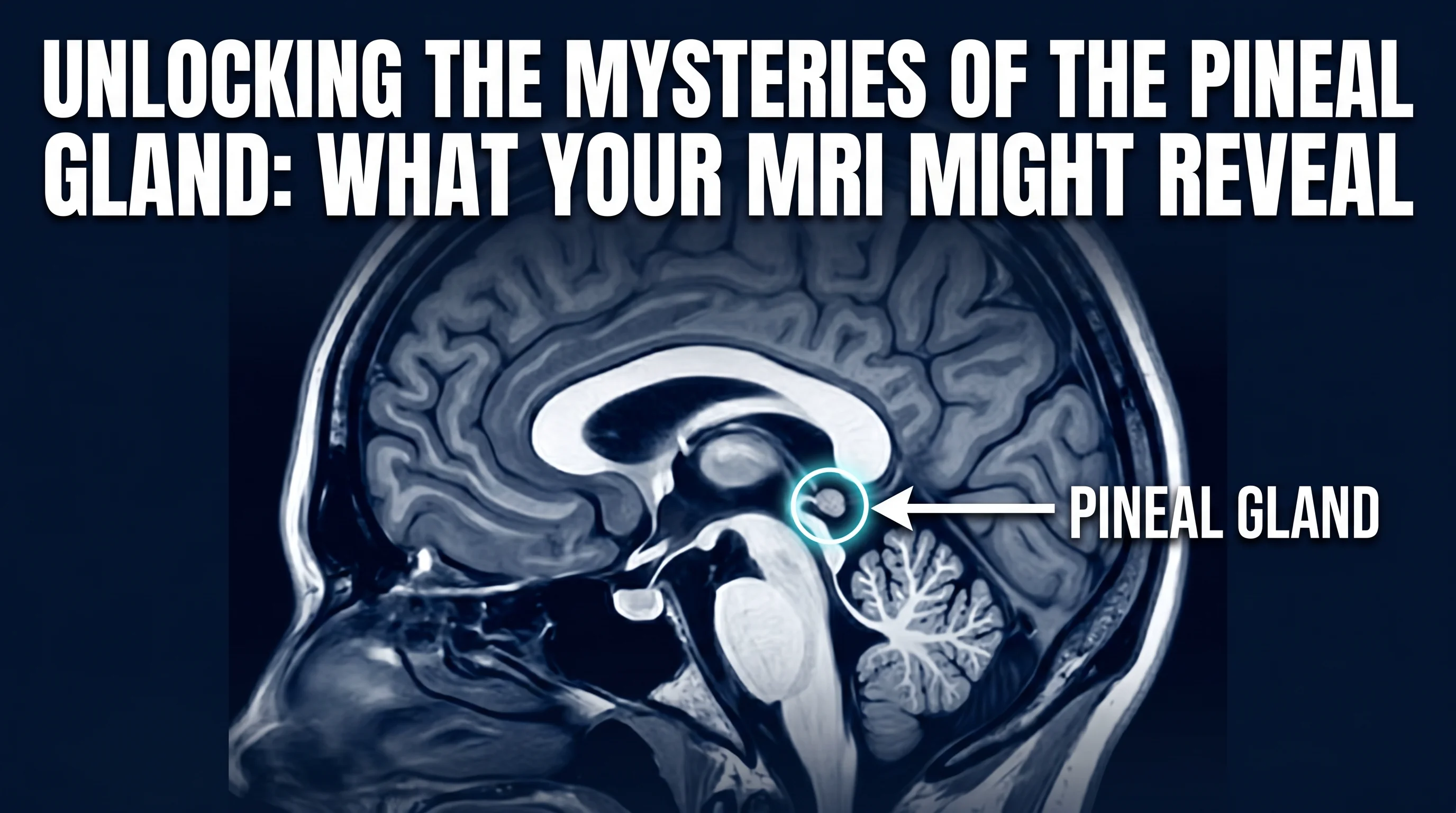
What Pineal Gland Calcification Actually Is
The pineal gland doesn’t calcify the way a pipe corrodes. It’s more deliberate than that — and stranger.
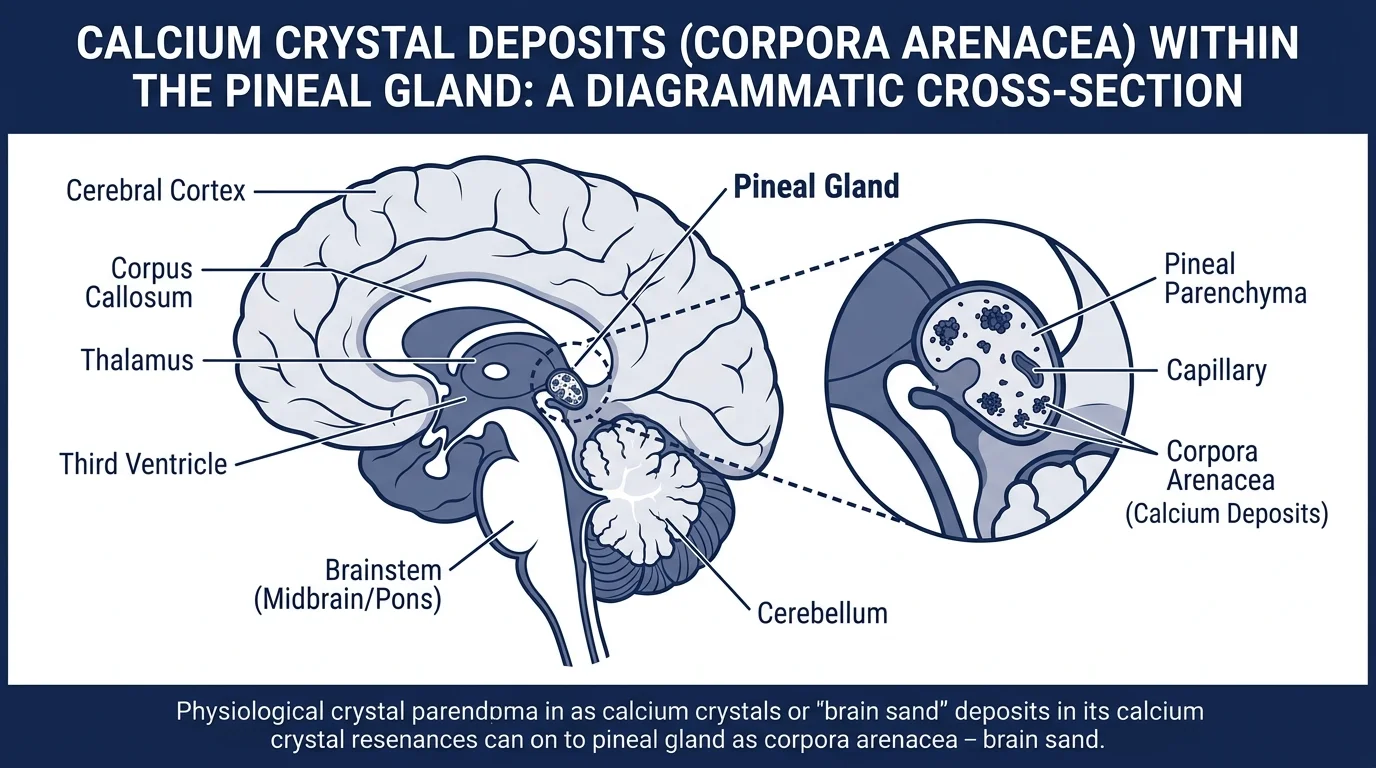
What happens: calcium phosphate crystals, known as corpora arenacea (or “brain sand”), accumulate within the glandular tissue over your lifetime. The process resembles bone formation mechanistically — involving mesenchymal stem cells and disruptions to calcium homeostasis within pinealocytes, as Tan et al. documented in their 2018 review in Molecules.
Why is the pineal gland so vulnerable? Because it sits outside the full protection of the blood-brain barrier. It’s a circumventricular organ — its capillaries are fenestrated, highly permeable, exposed to circulating minerals in ways most brain structures aren’t. A 2022 paper in Frontiers in Cellular Neuroscience confirmed this: the pineal receives some of the highest blood flow per gram of any tissue in the body, second only to the kidneys.
That’s a lot of circulatory exposure over a lifetime. It adds up.
Calcium phosphate crystals (corpora arenacea) accumulate in pineal tissue over decades — a process mechanistically similar to bone formation (Tan et al., Molecules, 2018).
As calcification progresses, it compromises the gland’s ability to synthesize melatonin. A 1994 postmortem study in the Journal of Pineal Research found that age-related declines in melatonin biosynthesis may directly reflect altered calcium homeostasis in the pinealocyte. Radiologists have used pineal calcification as a midline landmark in skull X-rays for decades — which tells you how predictable and prevalent it is, even before modern neuroimaging.
What Are the Symptoms of a Calcified Pineal Gland?
The most evidence-backed symptom is disrupted sleep — specifically insomnia and circadian dysregulation — linked directly to compromised melatonin output. Beyond that, the evidence gets thinner. Honesty requires saying that clearly.
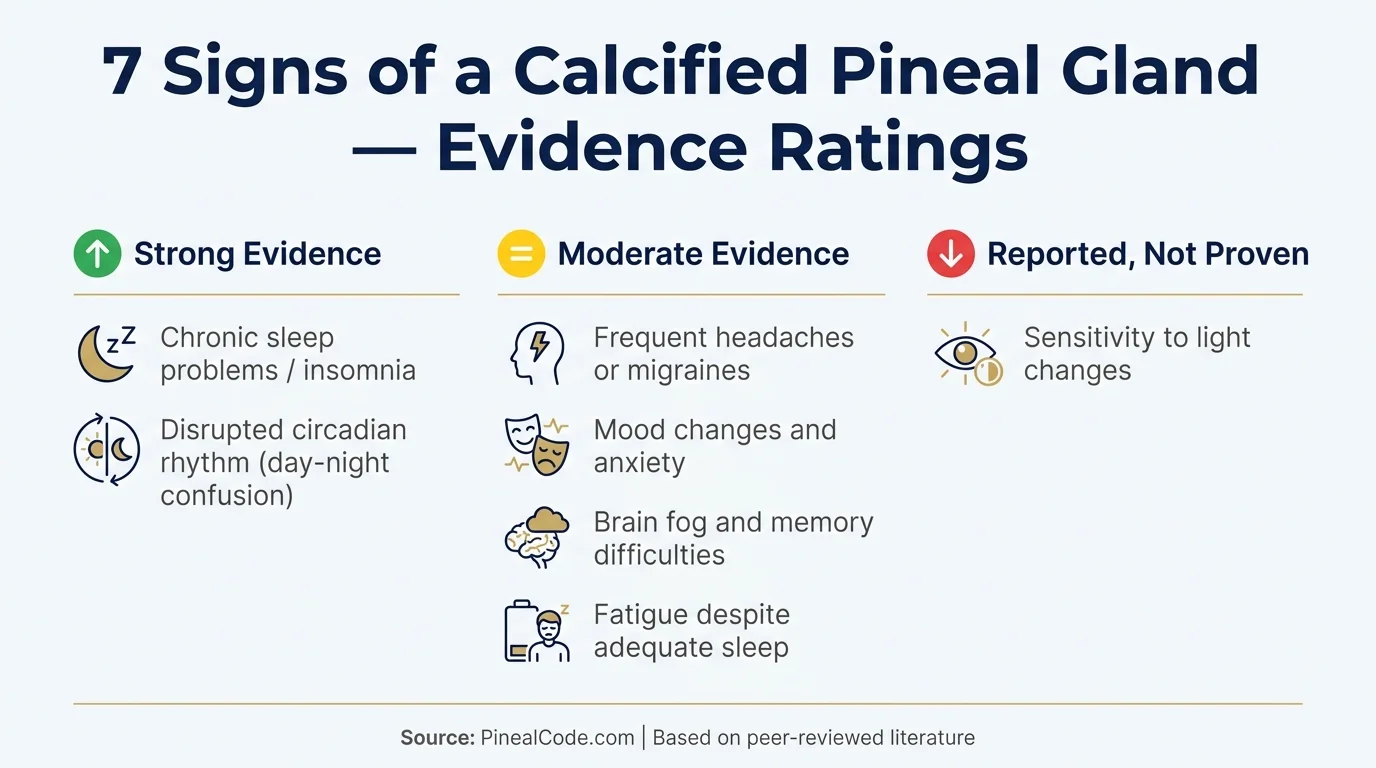
Here are the 7 most reported signs, each rated by actual evidence quality.
1. Chronic Sleep Problems and Insomnia 🟢 Strong evidence
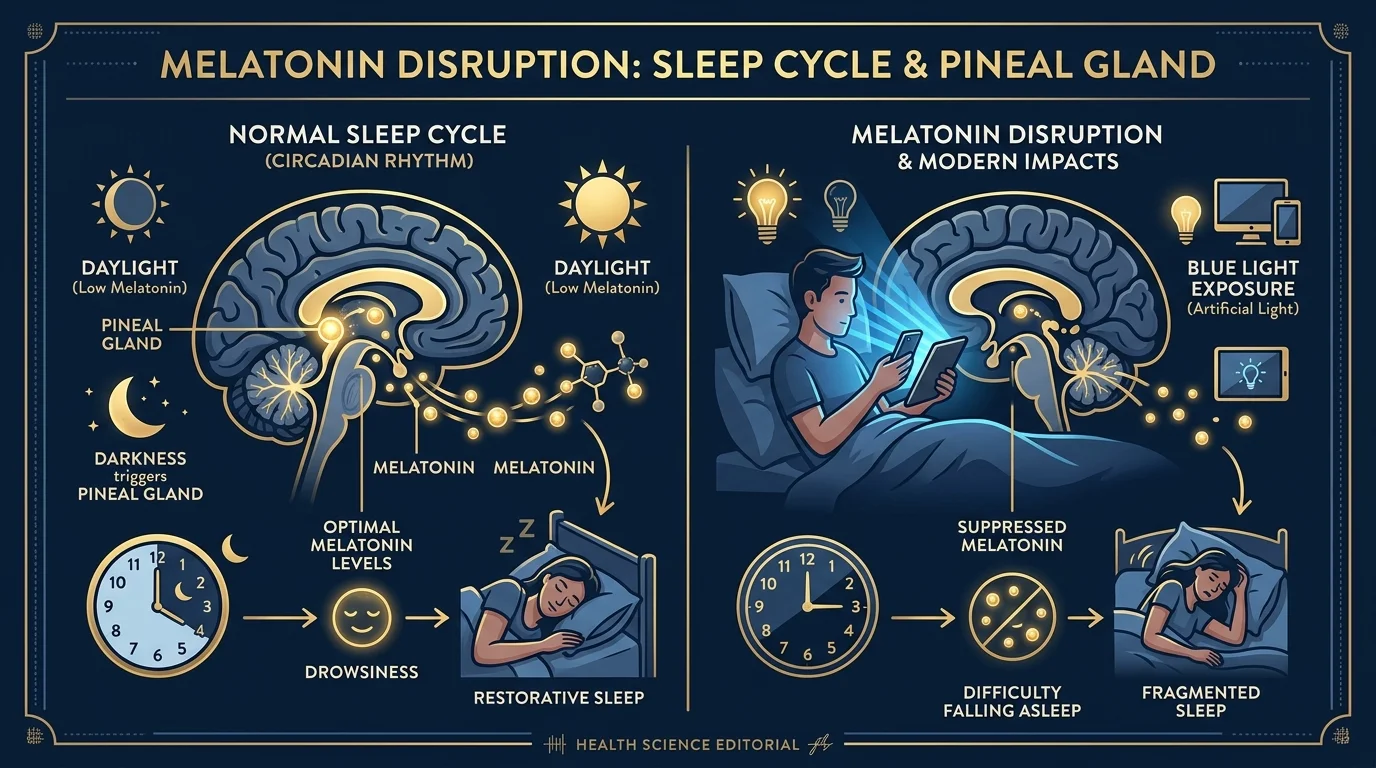
Melatonin is the mechanism. The pineal gland is the primary source, and melatonin drives the sleep-wake cycle. When calcification reduces functional tissue, output drops.
A 1998 pilot study by Mahlberg et al. in Pathophysiology (n=36) found that greater degrees of pineal calcification correlated with chronic, subjective sleep-wake disturbances. Daytime fatigue was the primary reported symptom. Small study. No randomization. But the mechanism is physiologically sound — it’s the same mechanism explaining why melatonin production declines with age, tracking the same trajectory as calcification prevalence.
If your sleep has deteriorated without a clear lifestyle explanation and you’re over 30, this isn’t something to dismiss. For strategies specifically timed around sleep cycles, see pineal gland decalcification at night.
2. Frequent Headaches or Migraines 🟡 Moderate evidence
Both the Cleveland Clinic and Molecules (Tan et al., 2018) reference a loose link between pineal calcification and migraines — specifically, that reduced CSF melatonin levels may contribute to neurological vulnerability underlying cluster headaches.
The mechanism isn’t established. Association is not causation, and there are dozens of reasons someone develops chronic headaches. But melatonin has documented analgesic and anti-inflammatory properties in the CNS. A gland producing less of it is a plausible contributor.
Plausible isn’t proven. Worth noting, not worth diagnosing.
Melatonin is synthesized from serotonin in the pineal gland and drives the sleep-wake cycle. Calcification that reduces functional tissue directly limits melatonin output.
3. Mood Changes and Increased Anxiety 🟡 Moderate evidence
Melatonin doesn’t operate alone. It’s synthesized directly from serotonin, and disruptions in melatonin cycling have downstream effects on mood regulation. Calcification that impairs melatonin synthesis may influence the neurochemical balance underlying anxiety and mood stability.
The operative word: may. The studies are associative. Nobody has run a controlled trial showing that addressing pineal calcification improves anxiety outcomes. What exists is a biologically plausible pathway and population-level correlations. That’s enough to take seriously — not enough to take as gospel.
4. Brain Fog and Memory Difficulties 🟡 Moderate evidence
This is where the Alzheimer’s research becomes relevant — and where precision matters most.
A 2006 study by Mahlberg et al. in Neurobiology of Aging examined 279 patients at a memory clinic. Alzheimer’s patients showed significantly less uncalcified pineal tissue (mean: 0.15 cm²) compared to controls (0.25 cm²; p=0.027). A 2019 review in Current Alzheimer Research (Bhowmick et al.) documented that progressive pineal calcification in AD patients tracks with cognitive decline and sleep disruption.
Here’s what the data doesn’t say: that calcification causes cognitive decline. Both calcification and neurodegeneration accelerate with age. In some individuals, they accelerate together. “Associated with” and “causes” are not interchangeable. That distinction matters a lot, and most articles in this space don’t make it.
If sign #1 is about sleep quantity, this is about sleep architecture. Without adequate melatonin signaling, the circadian clock loses its primary chemical anchor — falling asleep at wrong times, waking at 3am fully alert, groggy until noon regardless of how long you were horizontal.
The physiology is textbook. What’s less clear is the degree to which calcification specifically — rather than age-related melatonin decline from all causes — explains it in any given individual.
Downstream from signs #1 and #5. If pineal output is compromised, you may log 7–8 hours and still wake unrested — because the melatonin cycle governing sleep depth and REM architecture has been disrupted upstream.
The Mahlberg pilot study flagged daytime fatigue as the primary symptom in patients with higher calcification grades. Small study. Associative design. No causal claim. But the pattern fits the mechanism.
7. Sensitivity to Light Changes 🔴 Reported but not proven
This shows up frequently in forums and alternative health spaces. The logic isn’t absurd — the pineal gland receives photic input through the retinohypothalamic tract, and a compromised gland might theoretically alter that sensitivity.
No controlled studies link light sensitivity to pineal calcification as an isolated variable. It lives in anecdotal reports. That’s why it gets the red badge. I’m listing it because people report it consistently enough to acknowledge. I’m rating it red because honest is more useful than hopeful.
Evidence ratings across 7 reported signs: strong (mechanistically proven via melatonin pathway), moderate (associative studies), and reported but unproven in controlled research.
Who Is Most at Risk for Pineal Gland Calcification?
Age
Calcification rarely appears before age 10 — prevalence sits around 1.1–4.2% in early childhood. By age 18, that climbs to roughly 33%, according to a 1987 radiographic study in Rofo. The 2023 meta-analysis by Belay and Worku puts pooled adult prevalence above 61%.
The process accelerates through adolescence and early adulthood, plateauing around age 30. You don’t “develop” calcification in old age. You carry it forward from much earlier — which is the part nobody mentions.
Fluoride Exposure
The pineal gland accumulates fluoride. That’s not speculation — it’s documented in a 2001 study by Jennifer Luke published in Caries Research. Postmortem analysis found mean fluoride concentrations of 297 mg F/kg of wet pineal tissue. Higher than bone. The correlation between fluoride concentration and calcium in the gland was statistically significant (r=0.73; p<0.02).
Important limitations: n=11 cadavers, no functional data from living individuals, high inter-individual variability. But the finding has never been formally disputed in the peer-reviewed literature, and that says something. For the full picture, we cover all the fluoride data here.
Diet and Lifestyle
Additional factors in the literature: obesity, low-altitude environments, limited sun exposure, and potentially high EMF exposure — though the EMF data is considerably softer. An antioxidant-rich diet has appeared in preliminary research as potentially protective against oxidative stress in the gland — for a breakdown of specific foods with evidence behind them, see pineal gland foods.
Sex and Ethnicity
The 2023 meta-analysis flagged male sex and white ethnicity as correlating with higher calcification prevalence in qualitative analyses. Effect sizes weren’t dramatic, and the authors were cautious about confounders. Still a pattern that appears consistently enough to note.
How Is Pineal Gland Calcification Diagnosed?
Here’s what nobody says clearly enough: you cannot self-diagnose pineal gland calcification. The symptoms above are non-specific. Poor sleep, brain fog, mood shifts — that describes roughly 40% of adults for dozens of reasons that have nothing to do with the pineal gland.
Symptoms are a reason to investigate. They are not a diagnosis.
The confirmed methods:
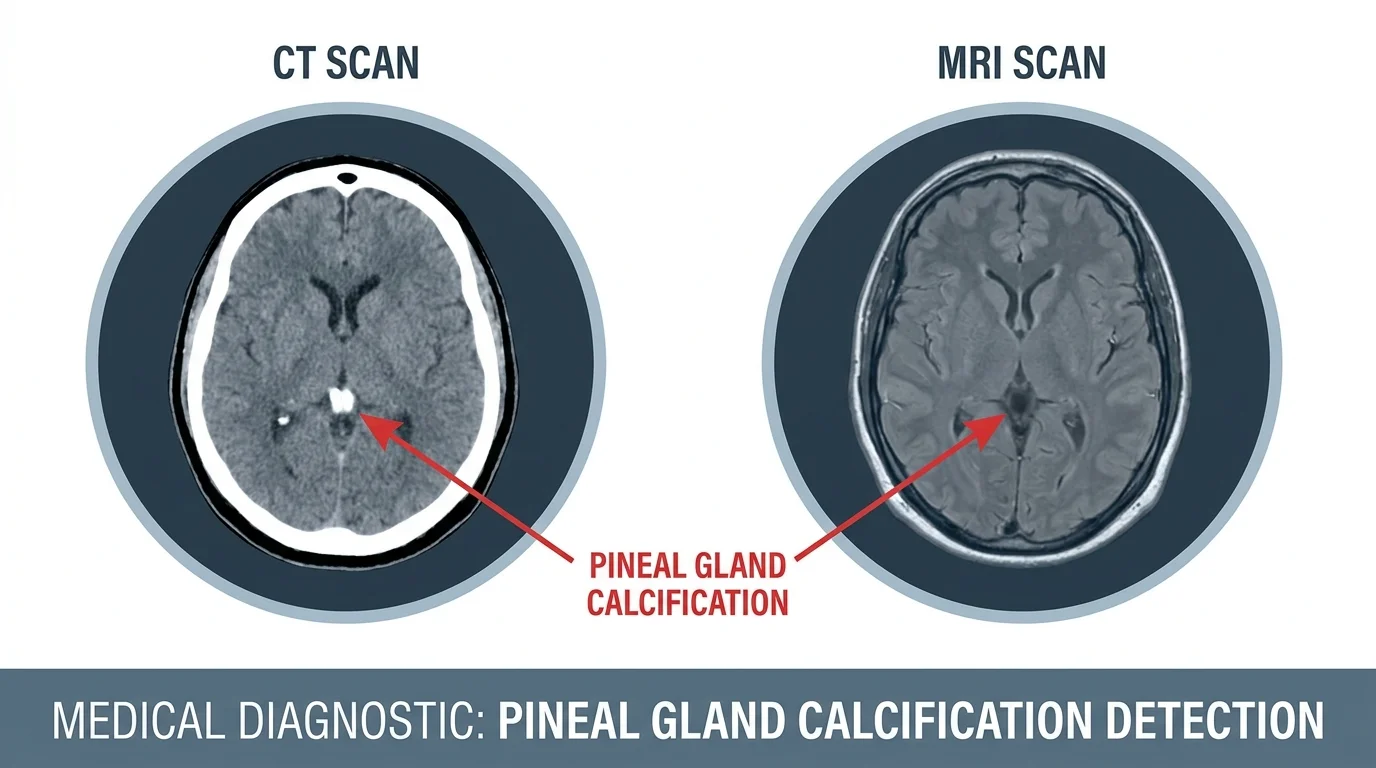
CT scan is the gold standard. Calcification shows up in the vast majority of adults on a standard cranial CT, often found incidentally — radiologists have used it as an anatomical landmark for decades precisely because it appears so consistently.
MRI with susceptibility-weighted imaging (SWI) is the most accurate alternative. A 2017 study in European Radiology (Seeger et al., n=384) found SWI reached 95% sensitivity and 96% specificity for pineal calcification detection — against 43% sensitivity for conventional MRI. No ionizing radiation, high accuracy. That gap is significant.
Lateral skull X-ray detects calcification in roughly 50–70% of adults. Lower sensitivity, but historically standard before CT.
Serum melatonin testing doesn’t confirm calcification. It can indicate functional impairment — but calcification grade and melatonin output don’t map onto each other linearly. How much functional tissue remains varies widely between individuals.
SWI-MRI reaches 95% sensitivity for pineal calcification versus 43% for conventional MRI — a significant diagnostic gap. CT scan remains the gold standard for routine detection (Seeger et al., European Radiology, 2017, n=384).
If you have persistent, unexplained sleep disturbance or cognitive changes you can’t account for, talk to a neurologist. Not a supplement stack. A neurologist.
What You Can Do Next
What we know: pineal calcification is common, measurable, and mechanistically tied to melatonin decline. What we don’t know: whether any specific intervention meaningfully reverses it in living humans. No randomized controlled trial has shown that. The research isn’t there yet.
That doesn’t mean nothing helps.
Reducing fluoride exposure (filtered water, fluoride-free toothpaste), prioritizing antioxidant-rich foods, protecting sleep hygiene, managing light exposure after dark — these are evidence-adjacent strategies that support the melatonin system regardless of calcification status. Not cures. Levers.
If you’ve already done the foundational work and want a targeted supplement, Pineal XT is one of the few formulations in this space built around the pineal gland’s documented biology — not vague “third eye” positioning. It won’t undo decades of calcification overnight. Nothing will. But if you want to support the gland running your melatonin production, it’s worth a look.
Quick Verdict — Pineal XT
4/5
Formulated around the pineal gland's documented biology — iodine for fluoride displacement, plus antioxidant compounds targeting the gland's high oxidative exposure. Lower price point than most competitors in this category. A reasonable option for those looking to support melatonin production at the source.
Supporting the pineal gland nutritionally works best as part of a broader protocol — filtered water, sleep hygiene, and reduced fluoride exposure included.
Frequently Asked Questions
Can you feel if your pineal gland is calcified?
Not directly. Calcification itself causes no pain or sensation. Some people associate symptoms like poor sleep or brain fog with it, but these are non-specific. The only way to confirm calcification is through medical imaging such as a CT scan or MRI.
What are the symptoms of a calcified pineal gland?
The most evidence-backed symptom is disrupted sleep and insomnia, linked to reduced melatonin production. Other reported symptoms include headaches, mood changes, and brain fog — but none of these confirm calcification on their own.
How is pineal gland calcification diagnosed?
A CT scan is the gold standard and can detect calcification in the vast majority of adults. MRI with susceptibility-weighted sequences reaches 95% sensitivity as an alternative. Blood tests for melatonin may indicate functional impairment but do not confirm calcification.
What age does the pineal gland calcify?
Calcification rarely appears before age 10. It increases rapidly through adolescence, reaching roughly 33% by age 18. Meta-analyses report an overall adult prevalence above 60%, making it extremely common in older adults.
Does fluoride calcify the pineal gland?
Research shows the pineal gland accumulates fluoride at concentrations higher than bone due to its limited blood-brain barrier protection. Studies associate fluoride exposure with increased calcification, though a direct causal mechanism in living humans is not fully established.
Is pineal gland calcification dangerous?
For most people, moderate calcification is a normal age-related finding. Excessive calcification has been associated — not proven as a cause — with conditions like Alzheimer's disease and migraines. See a doctor if symptoms persist.
Marcus Hale is an independent researcher and former clinical neuroscientist.
The content on PinealCode.com is for informational purposes only and does not
constitute medical advice.
Medical Disclaimer: The content on
PinealCode.com is for informational and educational purposes only. Nothing here
constitutes medical advice, diagnosis, or treatment. Always consult a qualified
healthcare provider before making changes to your health regimen.
Marcus Hale
Independent Researcher · Former Clinical Neuroscientist
I spent 12 years in clinical neurology before the questions got more interesting
than the answers. PinealCode is where I document what I find at the intersection
of brain science and consciousness.