NAC and the Pineal Gland: What 60 Years of Research Shows
By Marcus Hale·
Here’s a question I keep getting from readers who’ve already done their homework: “I know NAC raises glutathione. I know glutathione is an antioxidant. I know fluoride accumulates in the pineal. So — does NAC help?”
It’s a well-structured question. The logic holds. And the honest answer is: the mechanism is plausible, the direct evidence doesn’t exist yet, and anyone who tells you otherwise is confusing a hypothesis for a proof.
Can NAC decalcify the pineal gland? Not in any way that’s been tested directly. What it may do — and what the research does support — is a different, more precise claim. Let’s work through it.
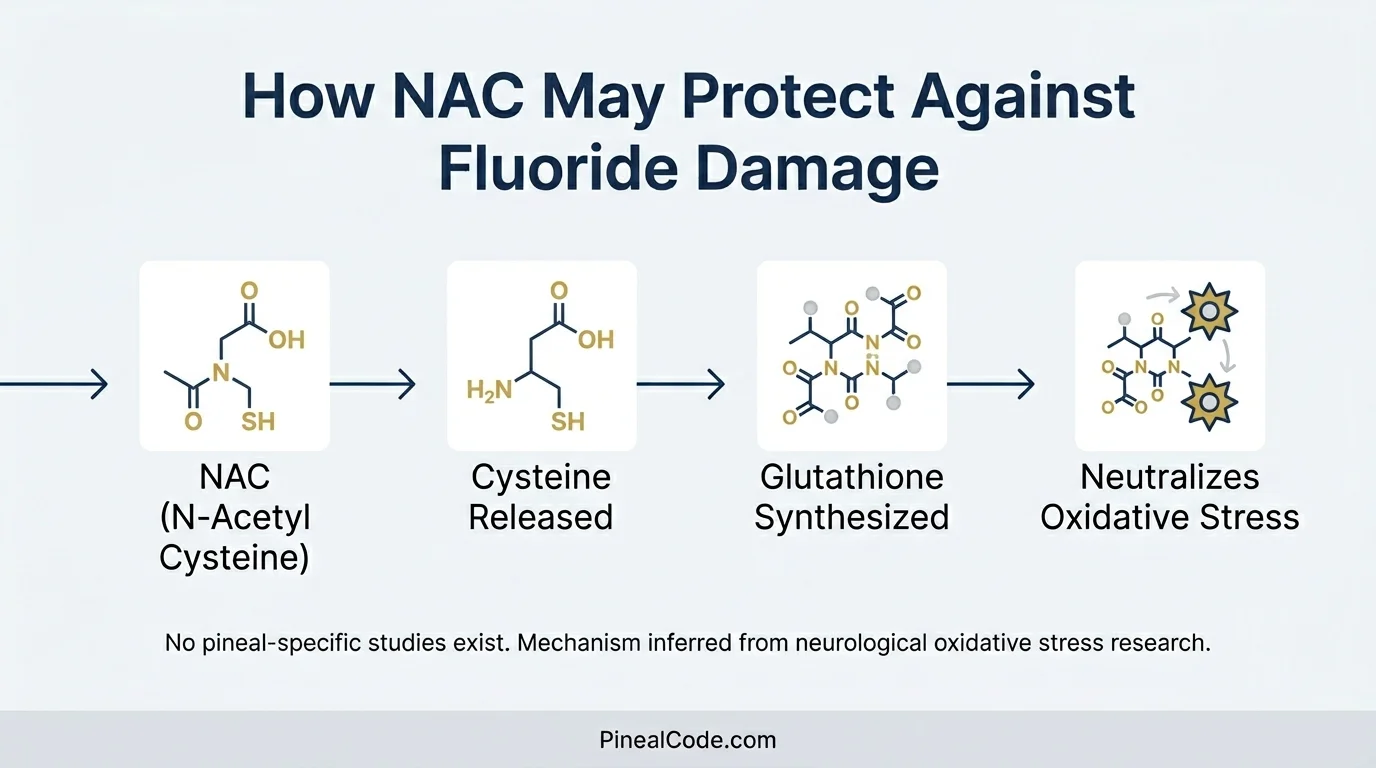
NAC supplies cysteine — the rate-limiting amino acid for glutathione synthesis — enabling cells to neutralize reactive oxygen species generated by fluoride accumulation. No pineal-specific studies exist; mechanism is inferred from neurological oxidative stress research.
What Is NAC and Why It’s Different From Most “Pineal Supplements”
NAC is N-Acetyl Cysteine. Precursor to glutathione — the body’s primary intracellular antioxidant — in clinical use since the 1960s. It started as a mucolytic and then became the standard emergency antidote for acetaminophen overdose — acetylcysteine is the standard treatment for acetaminophen overdose in emergency settings, with consensus guidelines recommending its administration within 8 hours of ingestion. When someone takes too much Tylenol and ends up in the ER, NAC is what goes into the IV line. That’s its origin story. Not a wellness product. A poison antidote that turned out to have much broader applications.
This is not a supplement that showed up in a biohacking forum last year.
Six decades of safety data in hospital settings. That alone makes it worth taking seriously when the mechanism question comes up — because when something has that kind of clinical track record, the question stops being “is this dangerous?” and starts being “does the mechanism actually apply here?”
The pineal angle emerged from a logical chain: NAC raises glutathione → glutathione has antioxidant and partial chelating properties → fluoride accumulates in the pineal and causes oxidative stress → therefore NAC might help.
Three links of inference. Each one needs to hold.
The Fluoride-Pineal Connection (What Established Science Says)
The pineal gland lacks a blood-brain barrier and receives approximately 4 ml/min/g of blood flow — second only to the kidney — which explains why fluoride accumulates there at concentrations comparable to teeth, not soft tissue.
That’s not a fringe claim. Jennifer Luke’s 2001 study, published in Caries Research, found that fluoride accumulates in aged pineal tissue at mean concentrations of 297 mg/kg wet weight — with individual hydroxyapatite samples reaching as high as 21,000 ppm and a statistically significant correlation between pineal fluoride and pineal calcium (r=0.73, p<0.02).
What makes the pineal uniquely vulnerable isn’t a flaw. It’s architecture. The gland sits outside the blood-brain barrier by design, meant to monitor what’s circulating in blood to regulate melatonin timing. That same exposure window that lets it read your bloodstream also means it absorbs what the rest of your brain is shielded from. I covered the full scope of what fluoride does to pineal tissue — and what it doesn’t if you want the complete picture before going further.
The pineal gland sits outside the blood-brain barrier and receives approximately 4 ml/min/g of blood flow — second only to the kidney — which explains why fluoride accumulates in aged pineal tissue at mean concentrations of 297 mg/kg wet weight (Luke 2001), comparable to mineralized teeth, not soft tissue.
Reddy et al. (2014), working with rat models, showed that fluoride exposure caused dose-dependent increases in lipid peroxidation and compromised antioxidant defenses in brain tissue, including a measurable drop in glutathione levels. The doses were higher than typical human exposure. That matters. But the core mechanism — fluoride generating reactive oxygen species, glutathione getting depleted trying to mop them up — is documented.
This is the problem NAC is theoretically positioned to address.
Here’s where the language needs to be precise, because it often isn’t.
Glutathione is not a classical chelator of fluoride. It doesn’t grab fluoride molecules and escort them out the way EDTA grabs lead. It neutralizes the damage fluoride causes — oxidative stress, membrane peroxidation, cellular inflammation. That’s a different job. Stopping the fire versus removing the fuel.
Pawłowska-Góral et al. (2013), published in Toxicology In Vitro, showed that NAC protected rat hepatocytes from fluoride-induced oxidative damage. When I first read that paper, I thought I’d found the mechanistic link I was looking for. Then I looked again: hepatocytes. Liver cells. Not neurons. Not pineal. I’d been reading what I wanted to find.
The extrapolation from liver cell to pineal gland involves several inferential steps that haven’t been tested.
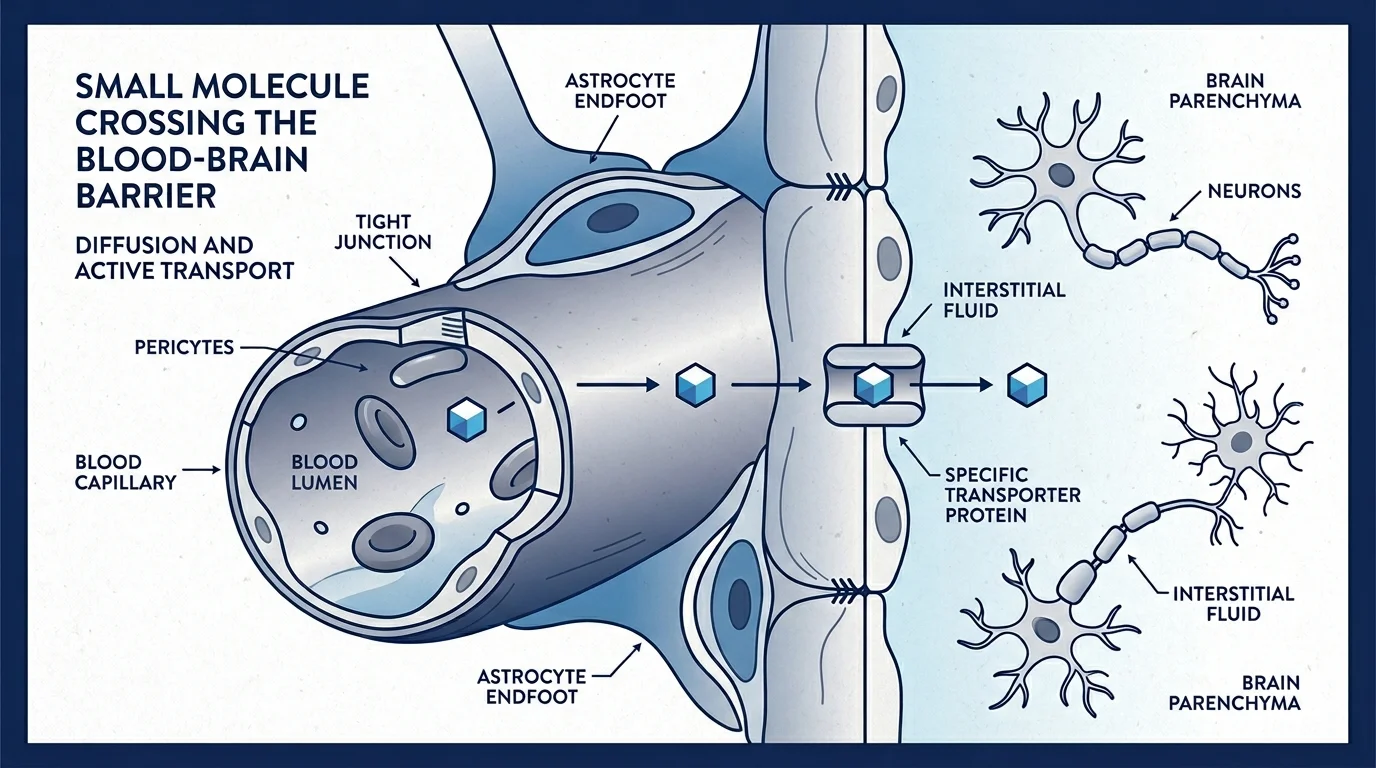
There’s a wrinkle here, though. The pineal gland is outside the blood-brain barrier already. So NAC’s ability to penetrate that barrier matters for surrounding brain tissue, but the pineal is directly exposed to circulating substances regardless. The argument for NAC reaching the pineal is actually simpler: if it’s in your bloodstream, the pineal sees it.
Unlike glutathione itself, NAC crosses the blood-brain barrier efficiently — confirmed across multiple neurological models including multiple sclerosis and psychiatric oxidative stress conditions. The pineal gland is outside the BBB regardless, meaning NAC reaches it directly via bloodstream.
What the Studies Actually Say About NAC and Pineal Calcification
Let me be direct about what the literature contains, and what it doesn’t.
NAC raises glutathione. Glutathione is depleted by fluoride-induced oxidative stress. NAC has demonstrated neuroprotective properties in multiple neurological contexts. A small but real 2021 trial (Shahrampour et al., Heliyon) showed it altered cerebral blood flow in MS patients — actual measured activity, in actual humans, in the brain.
None of that is nothing.
What’s missing: no study has tested NAC on pineal tissue. Not in animals. Not in humans. The gap between “NAC reduces oxidative stress in brain tissue generally” and “NAC decalcifies the pineal gland specifically” isn’t a small one. It’s the entire experiment that hasn’t been run.
This isn’t evidence that NAC doesn’t work on the pineal. Absence of evidence isn’t evidence of absence. The mechanism is plausible. And the downstream effects of that oxidative stress — disrupted melatonin synthesis, the sleep and cognitive symptoms that follow — are well documented even if the NAC connection isn’t.
But here’s what I keep coming back to: the biohacking community has correctly identified a real mechanism and then inflated it into a proof. That’s not science — that’s wishful extrapolation with good vocabulary. The mechanism is there. The study isn’t.
Can NAC Remove Fluoride From the Body?
Partially, and with caveats. Via glutathione’s antioxidant activity, NAC may reduce the damage caused by fluoride that’s already accumulated. Whether it facilitates actual fluoride excretion from pineal tissue is a separate, untested question. Fluoride binding into hydroxyapatite is a structural process. Antioxidants work on oxidative chemistry. Different problems, different tools.
What Dosing Researchers Have Used
The studies aren’t recommending doses to you or me. They’re testing mechanisms. With that on the table:
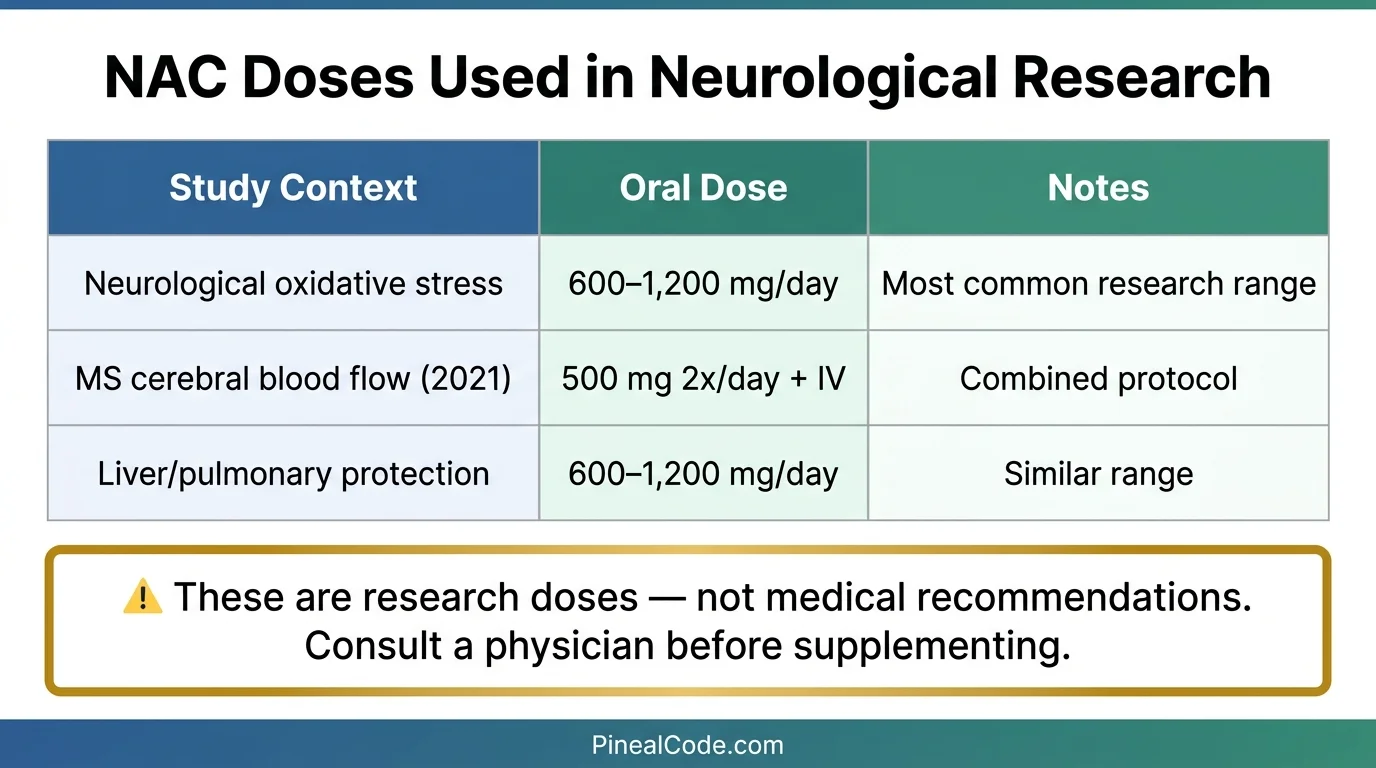
Neurological oxidative stress research has generally used oral NAC at 600–1,200 mg/day. The MS cerebral blood flow study (Shahrampour 2021) used a combined protocol: 50 mg/kg IV weekly plus 500 mg twice daily orally. Liver protection and pulmonary studies fall in similar oral ranges.
One thing worth knowing: oral NAC has low bioavailability, roughly 6–10% by most estimates. In controlled models, NACA restores 91% of endogenous GSH compared to only 15% with standard oral NAC — which is why researchers have explored ethyl ester forms as more absorbable alternatives. The IV route avoids the absorption problem entirely but isn’t realistic for self-directed use.
Not a dosing recommendation. If you’re considering NAC, that conversation belongs with a physician.
Research doses used in neurological oxidative stress studies — not clinical recommendations. Oral NAC has low bioavailability (~6–10%); NACA (ethyl ester form) restores 91% of endogenous glutathione versus 15% with standard oral NAC (Frontiers in Neurology, 2017). Physician consultation required before supplementing.
What NAC Can’t Do — The Honest Limits
If someone tells you NAC will definitely clear your pineal, they’re selling you a mechanism as a proof.
Calcification in the pineal gland involves hydroxyapatite — crystalline calcium phosphate deposits. That’s a structural change. No antioxidant reverses structural crystalline deposits. There is no imaging study, no CT, no MRI, demonstrating reduction of pineal calcification after any supplement: not NAC, not tamarind, not boron, not anything currently in the decalcification conversation.
What antioxidants may do is reduce the ongoing oxidative damage that accompanies fluoride accumulation. Whether that matters for pineal function is genuinely open. Melatonin synthesis happens in the glandular cells, not in calcified deposits. If oxidative stress is impairing those cells, reducing it could support function. But that’s several logical steps from “NAC decalcifies the pineal.” For a realistic picture of what reversal actually looks like — and what the evidence does and doesn’t support — the science on reversing pineal calcification is worth reading before committing to any protocol.
NAC may be preventive and protective. It is not a reversal agent for existing calcification — at least not in any way that’s been demonstrated.
NAC is one of the most clinically studied compounds in medicine — but the pineal-specific evidence gap is real. An informed decision starts with understanding what the mechanism supports (reduced oxidative damage from fluoride) versus what it doesn’t (confirmed decalcification).
Final Verdict — Worth Considering If…
NAC makes the most sense as part of a broader conversation about fluoride and oxidative stress. Not as a standalone pineal intervention.
If you’re already investigating this area, the supplement with the strongest direct evidence for fluoride excretion is tamarind — 37% increase in urinary fluoride excretion in human trials. Boron and K2+D3 appear in the literature with different but related mechanisms. NAC sits in a separate category: strong general evidence, plausible mechanism for the pineal specifically, no pineal-specific testing yet.
For someone already tracking fluoride exposure, paying attention to sleep quality, and looking at the full evidence picture — NAC at 600mg is a reasonable addition to evaluate, with a physician’s input. For someone expecting a dramatic shift in consciousness or a measurable change on pineal imaging: that expectation has no evidence behind it.
Start with sleep. If you want to do more, do it informed.
Frequently Asked Questions
Can NAC decalcify the pineal gland?
NAC has a plausible mechanism via glutathione-mediated reduction of fluoride-induced oxidative stress, but no study has tested it directly on pineal tissue. The evidence supports reduced oxidative damage from fluoride — not confirmed decalcification.
Does NAC cross the blood-brain barrier?
Yes. Unlike many antioxidants, NAC has documented cerebral bioavailability, which is why researchers have studied it for neurological oxidative stress conditions including multiple sclerosis and psychiatric disorders.
What supplements help decalcify the pineal gland?
The strongest direct evidence points to tamarind (37% increased fluoride excretion in human trials), boron, and K2+D3. NAC has a plausible mechanism but lacks pineal-specific studies. No supplement has imaging evidence of reversing existing calcification.
Is NAC safe to take daily?
NAC has 60+ years of safety data in clinical use. Doses of 600–1,200 mg/day have been used in research settings. Consult a healthcare provider before supplementing, especially if you take other medications.
Marcus Hale is an independent researcher and former clinical neuroscientist.
The content on PinealCode.com is for informational purposes only and does not
constitute medical advice.
Medical Disclaimer: The content on
PinealCode.com is for informational and educational purposes only. Nothing here
constitutes medical advice, diagnosis, or treatment. Always consult a qualified
healthcare provider before making changes to your health regimen.
Marcus Hale
Independent Researcher · Former Clinical Neuroscientist
I spent 12 years in clinical neurology before the questions got more interesting
than the answers. PinealCode is where I document what I find at the intersection
of brain science and consciousness.