How to Remove Heavy Metals from Your Pineal Gland Naturally
By Marcus Hale··Updated March 26, 2026
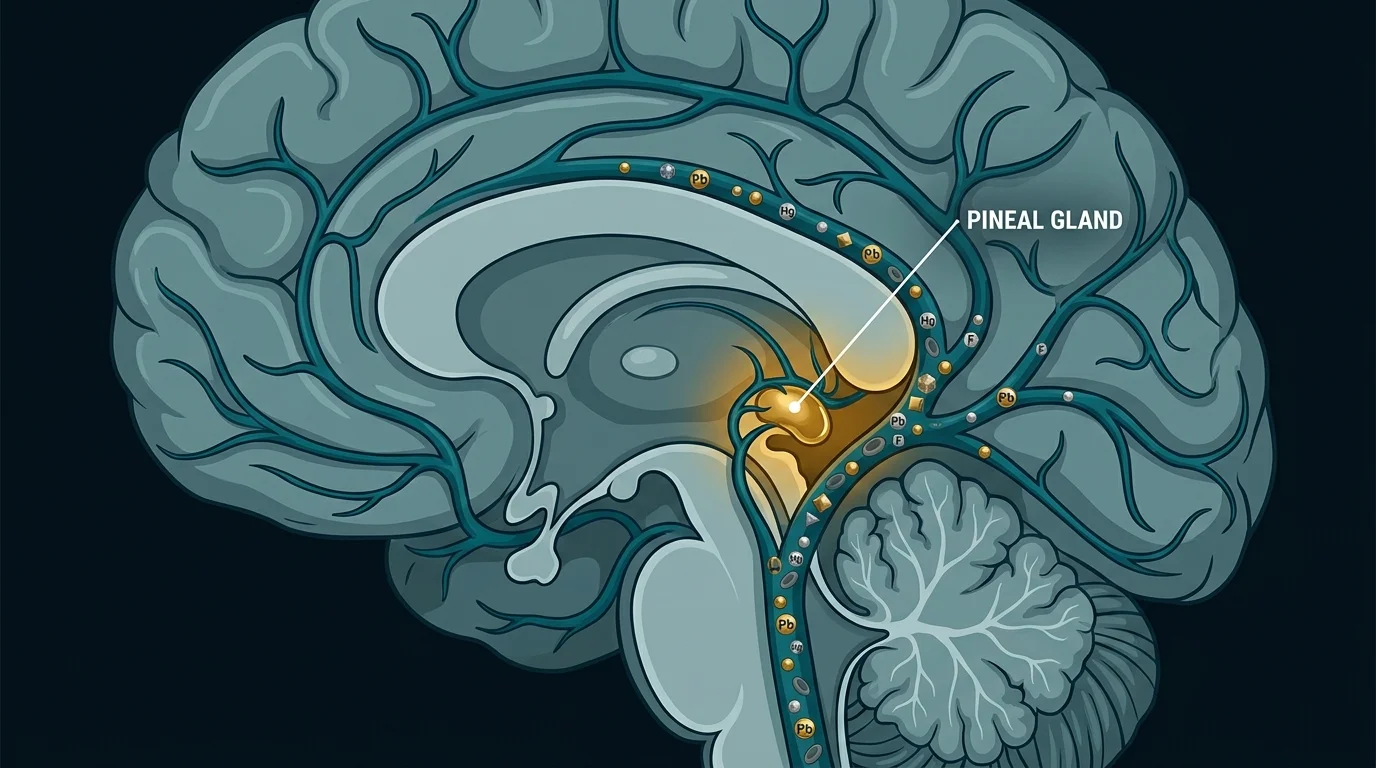
Your pineal gland sits behind the blood-brain barrier. Except it doesn’t, actually. That’s the thing most people get wrong. Most of your brain is protected by a tightly regulated vascular filter. The pineal gland is not. It’s one of the few brain structures that sits outside that barrier — one of a group of specialized structures known as circumventricular organs — bathed in blood flow second only to the kidney in terms of perfusion rate.
Which means whatever is circulating in your blood, including heavy metals, has direct access to it.
Learning how to detox heavy metals from your pineal gland naturally starts with understanding that this isn’t fringe biology. The accumulation is documented in peer-reviewed tissue studies. The gaps in the research are real too, and I’ll flag them as we go. What I won’t do is sell you a simple story about a gland that science is still working to understand.
Let’s start with what we actually know.
What Heavy Metals Accumulate in the Pineal Gland?
Multiple metals have been documented in pineal tissue: fluoride, lead (Pb), mercury (Hg), aluminum (Al), and arsenic (As). Of these, fluoride is the most thoroughly studied. The numbers are startling.
A 2001 study by Jennifer Luke published in Caries Research found fluoride concentrates in the pineal gland at roughly 9,000 parts per million in calcified tissue. That’s higher than in bone, which typically runs around 1,000 ppm. Not slightly higher. Nine times higher.
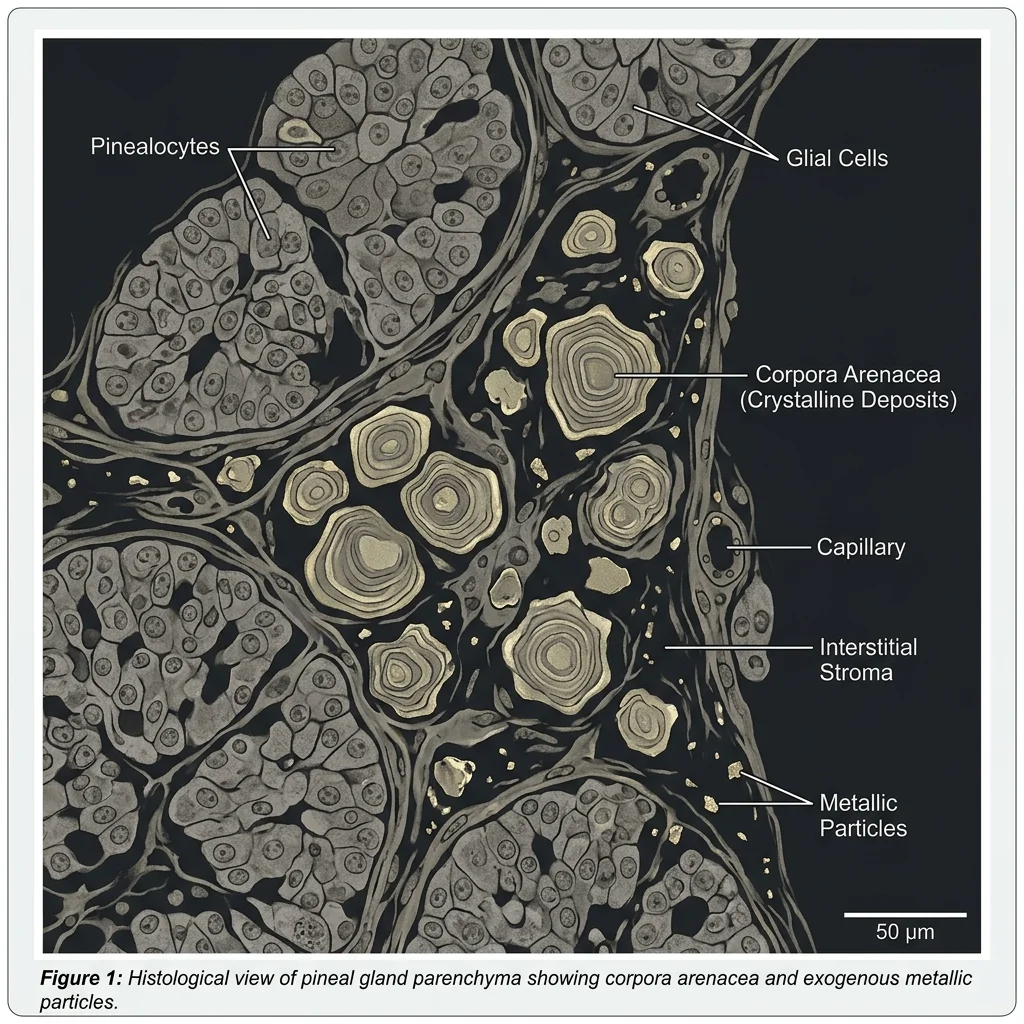
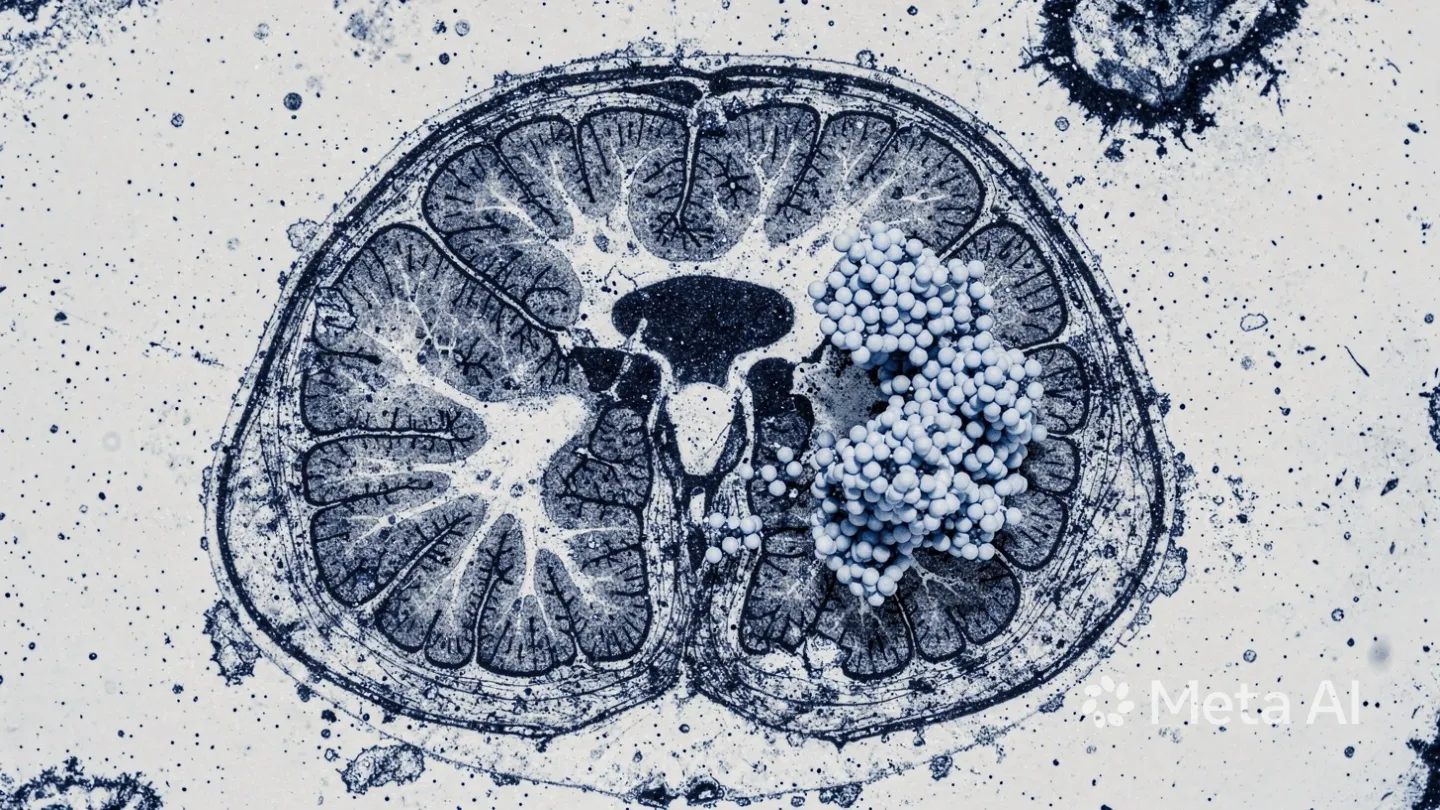
Baconnier et al. (2002) published in Bioelectromagnetics identified calcium-containing microcrystals in human pineal tissue, and the mineral composition suggests accumulation of external elements, not just endogenous calcium metabolism. More on those crystals at the pineal gland crystals article.
Mercury enters the picture through diet, primarily large predatory fish. A 2023 paper by Pamphlett and Bishop in Frontiers in Neurology used autometallography to confirm mercury deposits directly in pineal cells of individuals with high methylmercury intake. This wasn’t a theoretical model. These were actual tissue samples. Actual mercury. In the actual gland.
Why does the pineal accumulate more than other tissues? Two reasons: that missing blood-brain barrier, and the pineal’s exceptionally high blood flow. Toxins that circulate get filtered out of most brain regions. Here, they pool.
Pineal tissue cross-section showing crystalline deposits. The gland’s lack of a blood-brain barrier and exceptionally high perfusion rate make it uniquely susceptible to heavy metal accumulation — including lead, mercury, fluoride, and aluminum.
Can Heavy Metals Cause Pineal Gland Calcification?
Yes. And the mechanism is more specific than “metals are bad.” Lead and fluoride interfere with calcium metabolism at the cellular level, promoting the deposition of hydroxyapatite crystals in pineal tissue.
Fluoride accumulates in the pineal gland at concentrations up to 9,000 ppm in calcified tissue — nearly nine times higher than in bone, according to Luke (2001) in Caries Research — making it the most fluoride-dense soft tissue in the human body.
Grandjean’s 2019 review in Environmental Health confirmed that fluoride crosses the blood-brain barrier, reaches cerebrospinal fluid at concentrations approaching serum levels, and binds preferentially to calcium-rich tissues, including the calcified portions of the pineal. Heavy metals don’t just deposit passively. They actively disrupt the enzymatic regulation of calcium, accelerating a process the pineal is already prone to with age.
Here’s where I have to be careful. This is where the science gets inferential.
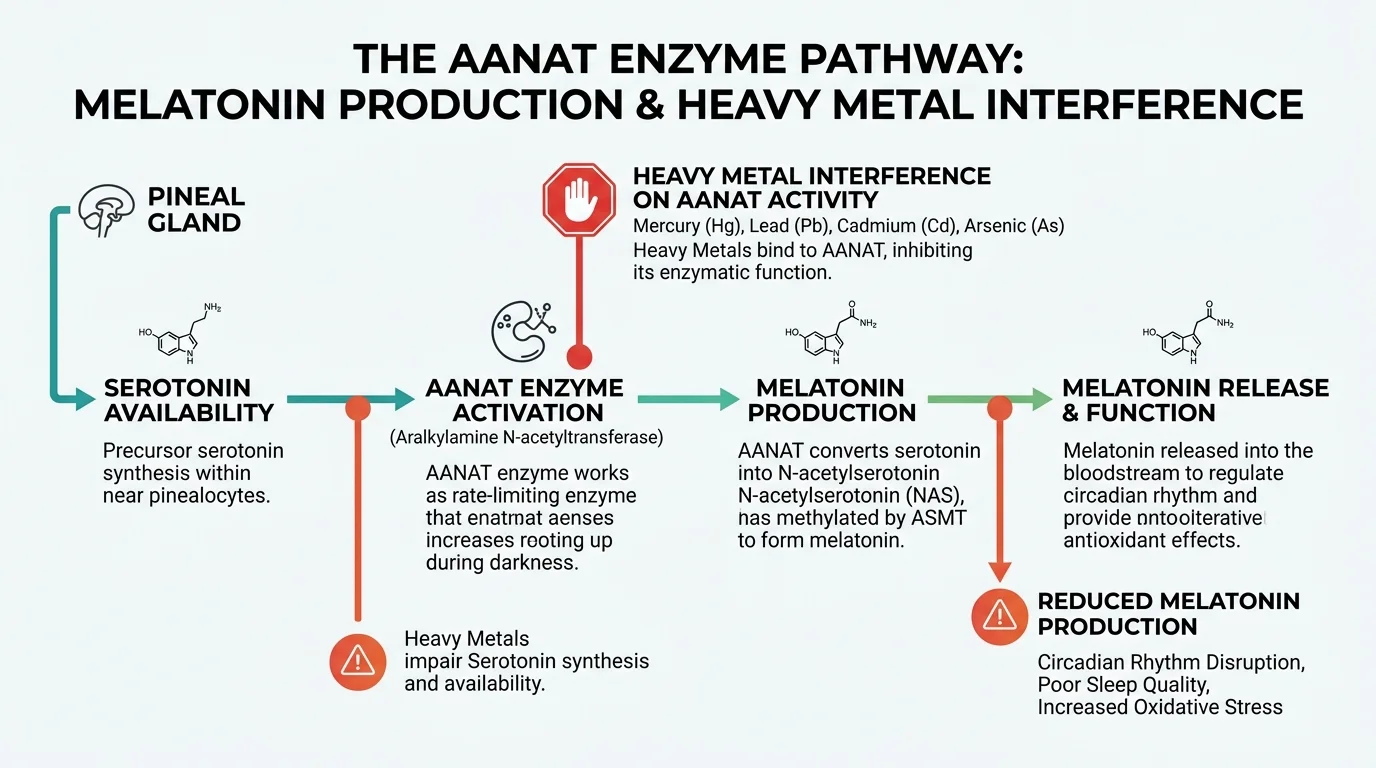
The pineal produces melatonin via a tightly regulated enzymatic cascade. The rate-limiting step is an enzyme called arylalkylamine N-acetyltransferase (AANAT). If AANAT gets inhibited, melatonin production drops. Full stop. Arendt and Aulinas (2022), in their Endotext chapter on pineal physiology, describe AANAT as the primary control point for nocturnal melatonin synthesis.
Here’s the gap I won’t paper over: no published study has directly demonstrated that mercury or lead inhibit AANAT specifically in human pineal tissue in vivo. I was at a functional medicine symposium a couple of years ago when a researcher cited this mechanism as if it were settled — it isn’t. What we do know is that heavy metals broadly inhibit enzymes that depend on thiol/sulfhydryl groups, and AANAT contains critical cysteine residues that fit that profile. The inference is mechanistically sound. It’s just not directly proven.
What is documented is the downstream effect. Disrupted melatonin means fragmented sleep. Less dream intensity. Shallower recovery cycles. Whether the mechanism runs through AANAT specifically or through broader oxidative damage to pinealocytes, the functional outcome is the same.
The AANAT enzyme controls nocturnal melatonin synthesis. Heavy metals inhibit thiol-dependent enzymes — and AANAT contains critical cysteine residues that fit that profile. The mechanism is plausible; the direct human evidence is not yet published.
How to Remove Heavy Metals from the Pineal Gland Naturally
No single intervention does this. What works is a layered approach: reduce incoming load, support binding and excretion, protect tissue while metals mobilize. In that order.
Foods That Chelate Heavy Metals Naturally
Cilantro is the most cited natural mobilizer for mercury and lead. I want to be precise here: the evidence for cilantro as a chelating agent is limited and methodologically uneven. The Georgiou (2018) trial with 347 foundry workers found that cilantro alone didn’t produce significant metal excretion in urine or feces. Where it showed promise was in combination, particularly with chlorella.
The detox world has turned cilantro into a folk hero. The reality is closer to “useful supporting character.” Honestly, that might be the most accurate endorsement any herb has ever received. Use it as a mobilizer. Not as a standalone chelator.
Chlorella + cilantro is the best-evidenced natural combination for heavy metal binding. Used separately, results are inconsistent. The Georgiou (2018) trial with 347 foundry workers showed meaningful benefit only when combined.
Chlorella binds metals in the gastrointestinal tract. When I first looked at the chlorella data, I expected to be disappointed. Another supplement with more marketing than mechanism. The GI binding evidence is actually decent. Merino et al. (2019), in Antioxidants, showed 90 days of supplementation reduced mercury, silver, tin, and lead levels in hair samples from patients with dental amalgams. Sample size was small (n=16), and chlorella was combined with fucus and aminosulphurates, not used in isolation. But the direction of effect is consistent, and the mechanism makes sense: binding in the GI tract, preventing reabsorption, reducing systemic load over time.
Spirulina has the broadest pre-clinical evidence base. Bhattacharya’s 2020 review in the Journal of Environmental Pathology covered 58 pre-clinical studies showing protective effects against arsenic, cadmium, lead, and mercury. Five clinical studies confirmed arsenic protection specifically. A 2023 in vitro study from Mallamaci et al. showed spirulina increased viability of neuroblastoma cells exposed to cadmium, mercury, and lead. Not pinealocytes, not humans in vivo, but directionally solid.
Wild blueberries aren’t chelators. They’re neuroprotective antioxidants, relevant because mobilizing stored metals generates oxidative stress. You want protection in place while metals are moving.
Supplements for Heavy Metal Removal
Chlorella (3–5g/day, food grade) is the baseline. GI binding, consistent daily use. Start here before adding anything else.
Modified Citrus Pectin (MCP) targets two things: metals and galectin-3, an inflammatory mediator involved in tissue fibrosis. Add it once the baseline is established.
Alpha Lipoic Acid (ALA). Stop here and read this carefully. ALA crosses the blood-brain barrier and can mobilize mercury, but if there’s no binding agent present to capture it, that mercury can redistribute to brain tissue rather than exit the body. This is documented in chelation literature, particularly in the Andy Cutler Protocol, which was developed specifically around high mercury burden cases. Use ALA only under medical supervision if you have reason to suspect significant mercury accumulation. Not optional advice. Not a footnote.
NAC (N-Acetyl Cysteine, 600mg) is a precursor to glutathione, the body’s primary endogenous antioxidant and indirect chelator. Safer starting point than ALA for most people, with fewer redistribution concerns.
Yes, there’s a supplement for that. There’s always a supplement for that. The difference here is the mechanism is real — just don’t skip source removal and expect capsules to carry the weight.
Does Chlorella Remove Heavy Metals from the Brain?
Chlorella does not cross the blood-brain barrier. It works in the gut, binding metals in the intestinal lumen, preventing their reabsorption into circulation, and reducing total systemic load over time.
That’s a critical distinction. If someone tells you chlorella “detoxes your pineal gland directly,” they’re extrapolating past what the evidence supports. The more accurate framing: by reducing how much mercury and lead is circulating systemically, chlorella reduces what the pineal is continuously exposed to. That’s indirect. It’s still meaningful. It’s just not magic.
The strongest evidence is for mercury and arsenic. Nakano et al. (2005) demonstrated chlorella’s ability to reduce methylmercury accumulation in animal models. The human data from Merino et al. (2019) points the same direction.
No study has directly measured chlorella supplementation against reduced metals in pineal tissue. I’d genuinely like to see that study. It doesn’t exist yet.
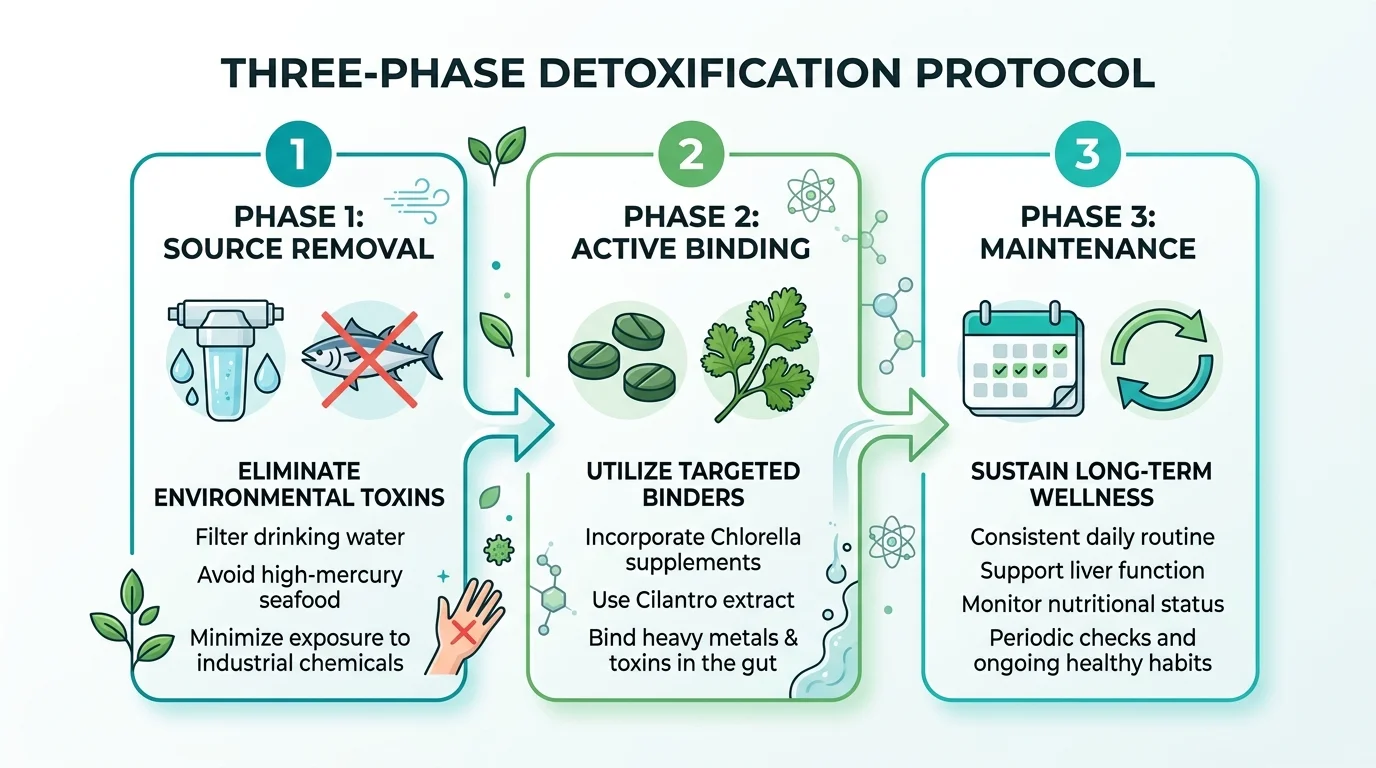
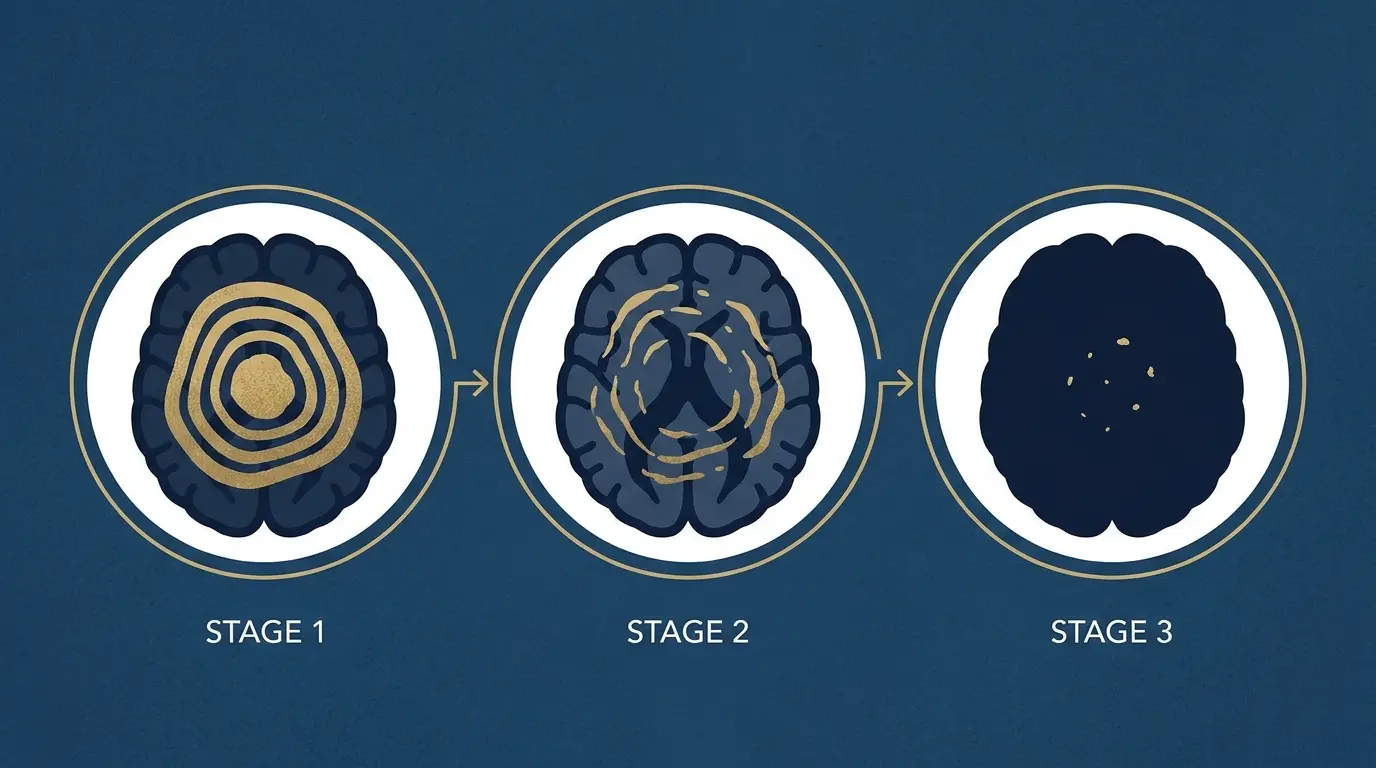
The 90-Day Heavy Metal Detox Protocol
Phase 1 — Remove Sources (Days 1–30)
Before you add anything, stop adding more.
Switch to reverse osmosis filtered water. This matters most for fluoride — standard carbon filters don’t remove it. Reduce or eliminate large predatory fish: tuna, swordfish, shark, king mackerel. These bioaccumulate methylmercury at concentrations that can meaningfully contribute to tissue burden with regular consumption.
If you have dental amalgam fillings, don’t rush to have them removed during this phase — improper removal generates acute mercury exposure. Consult a biological dentist who follows IAOMT protocol. Review personal care products for aluminum-based compounds, particularly antiperspirants and some antacids.
This phase isn’t dramatic. It just closes the tap before you try to empty the tub.
The 90-day protocol in three phases: close the source first, then bind actively, then maintain. Skipping Phase 1 and jumping to supplements is the most common protocol failure — you can’t outpace an open tap.
Phase 2 — Active Binding (Days 31–90)
Daily protocol:
Chlorella (3g) + fresh cilantro taken together — the combination shows more consistent results than either alone
Supplement stack: Chlorella 3g, Spirulina 2g, NAC 600mg. If you’re not under heavy mercury burden and have medical clearance, ALA 100–200mg can be added. Start low and do not take it on an inconsistent schedule. ALA has a short half-life; erratic dosing can cause redistribution between tissues.
Phase 3 — Maintenance
Once per month, run the cilantro + chlorella protocol for one to two weeks. Keep the filtered water permanent. Keep the large fish reduced.
Monitor indirectly: sleep quality, dream recall, and morning cortisol rhythm (how quickly you feel alert after waking). These aren’t perfect biomarkers for pineal function, but they’re what you can actually track without an MRI.
How Long Does It Take to Detox Heavy Metals Naturally?
Realistically: metals in active circulation can shift meaningfully in weeks. Metals stored in deep tissue, including bone, pineal, and organ depots, are a different category. We don’t have studies measuring clearance rates specifically from pineal tissue. What we can extrapolate from bone clearance data and other tissue depot research suggests months to years of consistent protocol for meaningful reduction in stored burden.
That’s not a comfortable answer. It’s an accurate one.
Set a 90-day minimum before evaluating. Expect gradual improvement in sleep architecture, not sudden transformation. Anyone promising faster results is selling something.
What This Means for You
Heavy metals accumulate in the pineal gland. This isn’t fringe biology. It’s documented in peer-reviewed tissue studies with identified mechanisms. The pineal’s unusual vulnerability comes from a specific combination: no blood-brain barrier, exceptionally high blood flow, and a calcium-rich microenvironment that pulls metals in.
Does accumulation directly cause pineal dysfunction? The chain is plausible but not proven in humans. We have tissue studies showing deposits. The relevant enzymes are inhibitable. Melatonin disruption affects sleep. But no clinical trial has closed the full loop — chelation protocol to improved melatonin to better sleep in a controlled population. That study hasn’t been done.
What we can say: reducing exposure and supporting natural excretion is low-risk and mechanistically supported. The protocol is gradual, not dramatic.
If you want to start somewhere, start with your water and your fish intake. Everything else is secondary.
Reverse osmosis is the only home filtration method that reliably removes fluoride. Standard carbon filters do not. Before any supplement protocol, this is the highest-leverage single change for reducing pineal heavy metal load.
Quick Verdict — Pineal Guardian
3.95/5
Nine botanical ingredients including Chlorella (heavy metal chelation), Tamarind (fluoride excretion), and Ginkgo Biloba (cerebral circulation). Liquid drop delivery for better absorption. Proprietary blend limits dose transparency, but the formula addresses the exact mechanisms covered in this article. 365-day guarantee.
Lead, mercury, aluminum, arsenic, and fluoride have all been documented in pineal tissue. The pineal gland lacks a blood-brain barrier, making it more susceptible to accumulation than most brain regions.
Can heavy metals cause pineal gland calcification?
Yes. Lead and fluoride are documented accelerators of hydroxyapatite deposition in pineal tissue. Heavy metals also disrupt calcium metabolism, promoting calcification.
Does chlorella remove heavy metals from the brain?
Chlorella primarily binds metals in the digestive tract, not the brain. It reduces systemic metal load by preventing intestinal reabsorption. Evidence is strongest for mercury and arsenic.
What is the best natural heavy metal detox?
The best-evidenced combination is cilantro + chlorella taken together, wild blueberries for neuroprotection, and removing sources first (filtered water, reduced large fish consumption).
How long does it take to detox heavy metals naturally?
Circulating metals clear in weeks. Metals stored in tissue (including pineal) require months of consistent protocol. Track sleep quality and dream vividness as indirect indicators.
Marcus Hale is an independent researcher and former clinical neuroscientist. The content on PinealCode.com is for informational purposes only and does not constitute medical advice.
Medical Disclaimer: The content on
PinealCode.com is for informational and educational purposes only. Nothing here
constitutes medical advice, diagnosis, or treatment. Always consult a qualified
healthcare provider before making changes to your health regimen.
Marcus Hale
Independent Researcher · Former Clinical Neuroscientist
I spent 12 years in clinical neurology before the questions got more interesting
than the answers. PinealCode is where I document what I find at the intersection
of brain science and consciousness.